Bill Gasiamis interviews Dr. Amir Hadanny, a renowned hyperbaric medicine specialist. Discover the incredible benefits of hyperbaric oxygen therapy for stroke recovery.
Learn More About Hyperbaric Oxygen Therapy (HBOT)
Dr. Shai Efrati on Hyperbaric Oxygen Therapy: A Game-Changer for Stroke Recovery
Hyperbaric Oxygen Therapy Improves Stroke Deficits
Bud Beucher: From Silent Survivor to Speaking His Truth Again
01:04 Introduction
03:21 Dr. Amir’s background in hyperbaric oxygen therapy
10:50 Funding a study on hyperbaric medicine
12:11 What is hyperbaric oxygen therapy?
14:13 Risks of having too much oxygen
18:59 What is hyperbaric oxygen therapy for stroke survivors?
24:24 Not everyone can do hyperbaric oxygen therapy
30:47 The proper hyperbaric oxygen therapy procedure
43:32 The four components of the protocol
50:59 The discovery of new blood vessels in the brain
1:05:56 Other field of study of Dr. Amir Hadanny
Dr. Amir Hadanny 0:00
You know, so we knew that hyperbaric medicine or hyperbaric oxygen therapy induces new blood vessels in those diabetic wounds. I’m going to share a slide here, that’s kind of critical to understand.
Dr. Amir Hadanny 0:15
This is a nice slide from the Weitzman Institute in Israel that was recently published. And what it shows, on the left side is how a wound in our leg or in our hand is healing. And on the right side is a wound in our brain, which is a stroke. And, you know, when I grew up, when I got my medical education, people have told me you cannot repair the brain. Nothing can. But we know today that is not true, we can repair the brain.
Intro 0:51
This is the recovery after stroke podcast, with Bill Gasiamis, helping you navigate recovery after stroke.
Introduction – Dr. Amir Hadanny

Bill Gasiamis 1:04
Hello, and welcome to episode 250 of the recovery after stroke podcast. On this episode of the show, we are joined by Dr. Amir Hadanny, a Harvard research fellow in the brain modulation lab to discuss hyperbaric oxygen therapy as an intervention for stroke recovery.
Bill Gasiamis 1:21
Dr. Haddany has a background in neurosurgery and bio informatics, with a particular interest in using machine learning to improve neuromodulation therapies. He has been leading the analysis of factory network mapping project, and will share his insights on how hyperbaric oxygen therapy can benefit stroke patients. We’ll discuss the science behind hyperbaric oxygen therapy and its potential to improve brain function and promote recovery after stroke. Dr. Amir Hadanny, welcome to the podcast.
Dr. Amir Hadanny 2:00
Thanks for having me.
Bill Gasiamis 2:01
My pleasure. Thank you for being here. Now, you’re the work that you do interests me a lot, because I’m a stroke survivor. And the podcast is called Recovery After Stroke Podcast and lots of stroke survivors do listen. And they’re looking for ways to support their recovery and to heal their brain after a stroke.
Bill Gasiamis 2:27
And one of the things that does come up from time to time and it doesn’t seem to be a lot of information about it is the kind of work that you do, which is in the space of oxygen therapy in the hyperbaric setting. And we hear about hyperbaric therapy, and we hear about how a whole bunch of people can get a tank and put it in their house these days.
Bill Gasiamis 2:51
It’s really developed a little further. But there’s still not enough information out there to inform the general stroke survivor, the general public about how beneficial that is, if at all. Now, I know you’re doing some interesting work in that space. Before we talk about that work. Can you give me a bit of a background on you? How you came to be involved in oxygen therapy. Give us a little bit of insight.
Dr. Amir Hadanny’s background in hyperbaric oxygen therapy

Dr. Amir Hadanny 3:19
All right, perfect. So a little bit about myself. So I trained as a neurosurgeon, and continue to do functional neurosurgery. And I also trained as a hyperbaric physician. I have a PhD in bioinformatics and data science, which really makes me a big data nerd.
Dr. Amir Hadanny 3:45
So I’m really all about data. That’s how I practice I have to have data in order to get actual clinical decisions. And the story behind and I guess most of the listeners would ask what does a functional neurosurgeon doing with hyperbaric medicine?
Dr. Amir Hadanny 4:04
And it all came down back in 2008. One of my MD instructors, who started managing a hyperbaric chamber, and I was doing my residency in neurosurgery. And he was treating diabetic patients for non healing wounds. So wounds in the legs for diabetic patients, that’s a common indication for hyperbaric oxygen therapy.
Dr. Amir Hadanny 4:36
And some of them had previous strokes and all of a sudden they reported you know, my speech is getting better. My hand is getting better. My leg is getting better. So he called me up after three patients and I tell him, I don’t know. I’m the skeptical, probably the most skeptical guy on the talk here and probably in the world.
Dr. Amir Hadanny 4:58
I told him no way. I don’t know about this. So after he collected it, several more patients, we decided we need to do a study, we need to do a randomized control study to actually see if there’s anything in this. So we started then I was excited because I wasn’t in my residency, I had patients who suffered from stroke that we treated, we gave them TPA, or thrombectomy, which is the endovascular intervention to try and salvage as much brain tissue as we can.
Dr. Amir Hadanny 5:37
But eventually, as you and your listeners know, there is some disabilities that you remain regardless of the treatment you’re getting. So I was excited that we may offer something else for our survivors. So we got them did randomised control trials.
Dr. Amir Hadanny 5:57
And the results were astonishing. The first study we did was on motor function, neurological function, and quality of life. And what we have shown that all the patients that we selected for this study, and I’ll touch on patient selection a little bit later, got significant improvements in their neurological function, and in their quality of life.
Dr. Amir Hadanny 6:28
And we compare this to a control group that did not receive that. And after the study was done, we crossed them over, meaning that the control group now received the treatment and got our protocol. And they improved just as much as the treated group. So that kind of nailed it down.
Bill Gasiamis 6:50
That makes me smile, because very often you hear in studies, the control group doesn’t get the benefit of the other people in the study, and they usually miss out and it’s a bit of a shame, I love the fact that they got to experience the same protocol. So before we talk about the protocol, and the different things that you discovered, is there a difference between a functional neurosurgeon and a standard neurosurgeon?
Dr. Amir Hadanny 7:24
Yes, yeah. So just to touch back on the last previous point, yeah, I have to touch on that both me and the Professor are really finding it hard on the ethical part that leaving the control group or the placebo group, untreated, so we always try to stick it in, in our health in keys or IRB reviews that we want to treat the control group if it works. So that’s what we usually do.
Dr. Amir Hadanny 7:55
Now the difference between a neurosurgeon and a functional neurosurgeon, so standard neurosurgeon treats trauma, and stroke, and brain tumors. A functional neurosurgeon specializes after that, after he completes that he specializes in functional disorders, such as movement disorder in Parkinson’s, or central tremor, or epilepsy or pain in try to improve the quality of life with different procedures or implementations of devices.
Bill Gasiamis 8:31
Okay, now, at the beginning, you also mentioned your data. So that meant that when you had people going into the hyperbaric oxygen chamber for diabetes, and three of them reported back that the neurological symptoms improved for you. That’s just it’s not real evidence. It’s just anecdotal evidence.
Bill Gasiamis 8:52
But it’s the type of evidence that should make your ears prick up and go, well, this is interesting, at least. And why are these three people reporting that. Is that how that process begins to start to evolve into a proper study? Is it that they came to you? Why is it that you guys hear that information and notice it from a number of people and then say, can we create some kind of study around this? How does it get from anecdotal to actually becoming a proper research thing?
Dr. Amir Hadanny 9:27
Yeah, I think that’s the I think that’s the natural history of science everywhere, right? It starts with a couple of case reports or that people collect data from different areas and then think, Okay, this is worth studying or not, at all at times, it’s by chance.
Dr. Amir Hadanny 9:47
So in our case, we had those three cases. And we looked in the literature to see if anyone else had encountered this we found several more case reports. So we decided Yes, it’s worth to check in, you know, making study conducting a study is really hard. It’s a human study a lot of people are doing, you know, you read it in the paper, this guy is found the cure for cancer, these guys found the cure to Alzheimer’s.
Dr. Amir Hadanny 10:17
And then when you read in line, you see it actually rat studies or mice studies, or pigs or rabbits, or you name the model, doing an animal study is easy. Okay, for two reasons. One, it’s cheaper, it’s easy to get the animals, it’s easy to conduct it when you doing human studies. It’s so complicated, it costs a lot of money. And it’s a lot of effort to get the patient to treat them, follow up with them.
Funding a study on hyperbaric medicine

Dr. Amir Hadanny 10:50
So it’s a big, big thing to do a study and especially in hyperbaric medicine, I think hyperbaric medicine is one of the fields that you don’t have any pharmaceutical company behind it. So there’s no funding, there’s no patent involved in it. So nobody’s going to give you the money to do with no money donated. So it’s really hard to do a study of hyperbaric medicine. So you have to have good anecdotes to persuade you. Okay, this is worthwhile studying that there is maybe something in it.
Bill Gasiamis 11:30
And who funds a study like that? If it’s the pharmaceutical companies are not behind it, is it a private funding? How does it get up?
Dr. Amir Hadanny 11:40
So usually, we go to the funds from the government and different scientific groups or private donations or the hospital funds, usually it’s the hospital investigations funds that help us to do it.
Bill Gasiamis 12:00
Awesome. Let’s get stuck into it tell me a little bit about this first, journey into hyperbaric oxygen therapy for stroke survivors. Tell me a little bit about that.
What is hyperbaric oxygen therapy

Dr. Amir Hadanny 12:11
Okay, I think that maybe we can start at what is hyperbaric oxygen, I don’t know, if you’ve covered it in previous podcasts.
Bill Gasiamis 12:20
Probably not, that’s a good place to start.
Dr. Amir Hadanny 12:24
Okay, so let’s go back to the concept of what’s going on. So we’re talking about a metal cage or a box or a room that’s built from pure metal. And people go inside of it, closing the door, and then we’re compressing air in it. So because it’s built with metal, the pressure inside of it goes higher and higher and higher.
Dr. Amir Hadanny 12:52
And then when we reach a certain level of pressure, each patient is given a mask, and he or she breathes 100% Oxygen. And then what it does, it basically increases the level of oxygen to a very high level that you cannot get with just a regular mask.
Dr. Amir Hadanny 13:19
People may ask when I have oxygen in the hospital, or an oxygen tank when I’m diving, but when they do it under pressure, you’re able to dissolve much more oxygen molecules in the blood, and then in the tissues in eventually in your brain. And we’re talking about 20 to 30 times more than what we have currently.
Dr. Amir Hadanny 13:44
So that’s kind of how it starts what’s going on when you’re being exposed to it. But the more critical part of it is, what happens if you do it repeatedly. So if you’re doing it over and over and over again on a daily basis, that’s when the therapeutic processes actually occur. And we can drill down to that a bit later if you’d like.
Risks of having too much oxygen
Bill Gasiamis 14:13
Yeah. Now, is oxygen always good for you? I’ve heard that oxygen can be bad for the brain as well. Too much oxygen in certain scenarios can be bad for the brain. Is that right?
Dr. Amir Hadanny 14:27
So obviously, if you have an acute event, let’s say an acute stroke or an acute myocardial infarction, on the first day or the second day of the event, usually you don’t want too much oxygen because when the damage is happening right on the moment the damage is happening. If you have too much oxygen, you can create some oxidants right you know about antioxidants obviously.
Dr. Amir Hadanny 14:58
But too much oxygen can cause oxidants and increase the injury actually. So you don’t want to have high oxygen at the moment of the injury. But let’s say several days afterwards, no problem, there isn’t really an issue of too much oxygen.
Dr. Amir Hadanny 15:18
However, you need to know how to do it, definitely, there are certain protocols, that if you’re going to get out of them or breach them, they can be toxic. If you’re getting to a very high level of oxygen, let’s say five atmosphere for atmospheres of pressure. If you’re trying to give oxygen you can cause oxygen toxicity, so definitely, you need to do it by a professional protocol.
Dr. Amir Hadanny 15:50
And know what are the limits of safe oxygen. If you breach them, you can hurt your lungs and hurt your brain. Lungs can deteriorate in pulmonary functions. And brain can actually cause seizures. So definitely there is something that’s called too much oxygen. So one of them if you’re doing it right in the event itself, but two if you’re doing unsafe protocols, you have to know what protocols you’re doing.
Bill Gasiamis 16:22
Is that a risk of people having an oxygen chamber in their home?
Dr. Amir Hadanny 16:29
Yes, definitely. That’s a big no, no, on my behalf, I think doing oxygen therapy at home is unsafe. For several reasons, one, yes, you can actually cause oxygen toxicity. If the chamber can actually get to those levels. And obviously, if something goes wrong, and you’re alone, there’s nobody that’s gonna save you.
Dr. Amir Hadanny 16:59
And unfortunately, there have been accidents and those kinds of sacs are chambers. So you know, even a spark caught fire and then, we’re not just dealing with a stroke survivor. So that’s on one end. But the more problematic side of this is that efficacy.
Dr. Amir Hadanny 17:26
A lot of people go in to those chambers or sacs and doing okay, I’ll do something. But they’re not following any protocol that has been studied they’d just go “Oxygen is good for you, let’s go in.” That’s not how it’s done. You can consider oxygen therapy, just like any other drug, it’s not like you will go into CVS right now and say I’ll take this drug every now and then right, you need to be prescribed a certain protocol, and you need to do it at the right timing, at the right amount, right pressure.
Dr. Amir Hadanny 18:03
And if you’re not doing this, nobody knows if it’s effective or not. So it’s kind of taking medicine to your own hands, which I really don’t like, if you want to do it, if you want to do oxygen therapy, do it with a professional and do it in the right way. With the right protocols that were investigated, improved. In a randomized control trial. That’s what being a data nerd is all about. You have to do based on data and you have to do medicine based on data.
Bill Gasiamis 18:35
Yeah, fair enough. I completely agree. And there is a proliferation of those home tanks, and they cost a lot of money. AUD Australian dollars, they start probably at around $20,000 Australian and then they take up some space in your home, and then you’ve got to get in them and you’ve got to go through that process.
What is hyperbaric oxygen therapy for stroke survivors?
Bill Gasiamis 18:59
I imagine that they become similar to treadmills, everyone buys a treadmill, they put it in their garage, and they start hanging the clothes on it so that the clothes can dry instead of run on it. I imagine it’s something like that, but I’m hoping that it’s starting to get looked at as a more serious medical intervention to help people that have a stroke. Is the field fairly new, or is it a field that has been around for a little while?
Dr. Amir Hadanny 19:36
So hyperbaric oxygen therapy, or hyperbaric medicine is already more than 70, 80 years old. And because it started from diving accidents. The whole field started by treating divers who breached protocols of diving and the only way to help them from their symptoms it’s called decompression sickness is going into a hyperbaric chamber.
Dr. Amir Hadanny 20:04
After that started, people realized we can heal those diabetic wounds or non healing wounds. So that’s been going on again for 50 or 60 years now. But the part for neurological patients neurological indications, including stroke, that’s pretty new.
Dr. Amir Hadanny 20:28
That is something that Professor Friday and myself are leading the investigations and the studies on it and the protocols to do it. Like I said, from 2008, before 2008. No data was there, other than anecdotes? So we took it to the next level of, okay. Let’s actually study this, let’s show what’s going on, do we get benefit from it? And what’s the mechanism behind it? So we talking about anywhere between 13 to 14 years old field, I would consider it rather new. And I think the potential is just getting started.
Bill Gasiamis 21:16
Yeah, 13 to 14 years ago. I mean, it’s very new. I mean, I had my first brain hemorrhage in 2012. And in 2012, podcasts really weren’t a thing yet. You know, the internet was just getting started, there was a lot of lack of information out there, and there was a lack of us, the stroke survivors being able to access that kind of information.
Bill Gasiamis 21:43
So it’s fairly new, I would imagine, but that’s good that, it’s been happening since 2008. I imagine you’ve got some good data by now. You’ve got some proven therapies by now. And you’ve helped a lot of people tell me a little bit about the actual work that you are doing and the things that you’ve discovered.
Dr. Amir Hadanny 22:04
So, like I said, the first study that we’ve done, we tested neurological function, motor function of patients with different neurological deficits. And we showed that we can actually improve motor function, as well as speech function, you know, people who have their areas of speech affected by bleeding or ischemia from the stroke, can lose their ability to talk.
Dr. Amir Hadanny 22:33
So we show that we can regain a lot of those capabilities back. The next study is focused on cognitive function. I don’t know if people know this, but apparently, up to 50% of stroke survivors suffer from cognitive deficits, whether its attention, or memory or processing speed, is slowed down significantly.
Dr. Amir Hadanny 23:04
Because you know, people think about stroke, okay, it’s just his hand or his just in his leg. But a lot of times, it’s all about cognition, that he’s not the same person anymore, he cannot go back to work because his brain doesn’t work the same to us so definitely, we focused on cognitive function.
Dr. Amir Hadanny 23:24
And we showed we are able to improve all the cognitive domains, like I said, memory, attention, executive function, processing, speed, coordination, we can regain a lot of the capabilities that were lost. Afterwards, we wanted to understand, does it matter what type of stroke you got?
Dr. Amir Hadanny 23:50
Obviously, there are different types. There’s ischemic ones when you have closure or clusion of an artery, and you have the hemorrhagic ones, like you mentioned, you had where the artery actually is ruptured. And also, you can have it in different areas of the brain. And you can have it in your dominant side or your non dominant side, we know that most people are their left hemisphere is dominant.
Not everyone can do hyperbaric oxygen therapy
Dr. Amir Hadanny 24:24
So if you have a right stroke, or left stroke, does it matter for our results? So we studied we spent a lot of times studying this and we found for most of it, it does not matter, it does not matter where you had stroke. And the reason for that is how we select patients.
Dr. Amir Hadanny 24:24
And I think that’s the critical part that I want to convey here. A lot of people, they’re doing hyperbaric oxygen therapy, whether they’re doing at home or clinics. The real thing is how you determine if a stroke survivor fits the treatment, if the treatment will actually benefit for it.
Dr. Amir Hadanny 25:11
So you have to do evaluations. So all of our patients go to specific evaluations that include cognitive assessments, physical assessments, and imaging. And in the imaging, we do two specific modalities, we do the MRI, that I’m sure a lot of people know about, which can tell us the anatomy of the brain, where the stroke was, what kind of damage happened there.
Dr. Amir Hadanny 25:46
But then on top of it, we’ll do another assessment called a SPECT scan, SPECT scan measures the function of the brain, or the metabolism of the brain. So we measure on each area of the brain, how much metabolism it works, and how much think about how much glucose it’s eating right now, to determine if this area is completely destroyed, or its normal functioning, or it has very low function that we can restore.
Dr. Amir Hadanny 26:23
So we want to work on areas that have low function, but not completely destroyed. Those are the areas that we can bring back to life or bring back to function. So during our evaluations, we look at the brain and we look, do we have those areas? We call those brain wounds or brain numbers, these areas? If we see them, then we know that, okay, we can improve those areas.
Dr. Amir Hadanny 26:55
But we need to know where are they located? And how do they correlate with the patient’s symptoms? If they’re in areas that if we will regain function, will it help the clinical symptoms. So that’s the evaluation that has to be done has to be done in order to determine if we’re going to help the patient, if that’s being done, appropriately. And if we select the patients, based on their on the imaging pay compared to the symptoms, then it doesn’t matter what type of stroke hemorrhagic is dynamic, and what’s the location of it and dominant and non dominant.
Dr. Amir Hadanny 27:45
All that matters is that you selected it correlated to the symptoms to those low metabolism areas. So again, take home message, patient selection, you have if you’re gonna do hyperbaric oxygen therapy, you have to do it in a place that’s doing evaluation and determines if it’s going to help you or not, not like oh, I’m a stroke survivor, let’s go in, not that.
Bill Gasiamis 28:12
I understand. Okay, so not everyone is going to be a candidate for hyperbaric oxygen therapy.
Dr. Amir Hadanny 28:22
I correct a lot will. Some of the patients are not some of the patients are at the point that it’s not going to work. And when you think about it, that’s how medicine always works. You have a treatment, it works for a significant portion of the patient.
Dr. Amir Hadanny 28:44
But on some it won’t, and you have to do this patient selection, because if you’re going to treat everyone, it’s never going to work. Think about acute stroke. When patients arrive to the hospital either getting a TPA or an endovascular intervention, we do patient selection, not everybody can have those procedures, depending on their time on the imaging on a lot of things, because we cannot do it for everyone. So patient selection for this medical intervention is critical.
Bill Gasiamis 29:17
Yeah, fair enough. Makes complete sense. And that’s kind of one of the issues with getting your own tank, putting it in the house and not having been evaluated by anybody for any reason. You might invest $20,000 in something that provides certain number of risks at home anyway, but then also maybe completely ineffective.
Dr. Amir Hadanny 29:41
Right, completely. It’s, a medical intervention, you have to do it with the professionals. I think people should really understand what they’re doing. It’s taking medicine into their own hands. They shouldn’t do it like like any other intervention, like they wouldn’t do an endovascular intervention on themselves, because they think they just now have a stroke is the same thing. It’s unsafe, and it may be uneffective. And it may be dangerous, so don’t do it.
Bill Gasiamis 30:15
Fair enough. All right. So the disclaimers are out of the way everyone has been forewarned. All right, so then, with the particular study, you guys selected your group, and then And then what happened? How did you go through the process? And, talk me through that.
Dr. Amir Hadanny 30:39
Okay, so are we talking about the study or a flow of a regular patient right now?
The proper hyperbaric oxygen therapy procedure
Bill Gasiamis 30:47
Yeah you take me through the process? I don’t really know. I want to learn you take me through the process. I’m very happy for you to guide the conversation. Yeah, for sure.
Dr. Amir Hadanny 30:56
Sure. So when we evaluate the patient, so patient comes in, and it can be two months after a stroke, or it can be 10 years after a stroke. I always tell patients, we need to do evaluations, I cannot determine if it’s going to help you or not, based on looking at you. Again, I need to do actual medical investigation.
Dr. Amir Hadanny 31:22
So the patient comes in, we see them, we evaluate them, we do a medical intake, we do physical examination, neurological examination. And then we start with a cognitive assessment. So they usually go and sit with a neuropsychologist, they sit in front of a computer and solve these, you know, games, you can call them, but they’re actual cognitive tests.
Dr. Amir Hadanny 31:48
Testing the memory, or their attention and all the cognitive domains. It’s all being done objectively on a computer. And then they meet up with a physical therapist, that again, tests everything, the range of motion and their the growth strength, and the reflexes, everything that we do, and their gait, everything that’s related to their injury, and overall neurological status.
Dr. Amir Hadanny 32:15
Then the patient also goes to the imaging facility where they go and have their MRI. So an MRI, very similar to a CT scan that a lot of the people here know about, lie down in the scanner, makes a lot of noise for 40 minutes or less, maybe 20 minutes, get their brain scan. And then they move to the SPECT scan, which is a very similar machine.
Dr. Amir Hadanny 32:45
Usually we inject some tracer into the veins, and then they’re being scanned about 40 minutes afterwards. Patient goes home, we process the data for about two, three days, we want to make sure we have everything, all evaluations, each professional writes up the report and their summary because we want it to be multidisciplinary. So we meet up the physician, the neuropsychologist, the physical therapist, the dietitian if we think there’s value for diet here.
Dr. Amir Hadanny 33:26
And we talk about what each of us saw and the impression, what was it, and then the physician looks at the imaging. And what we do in the imaging, we have specific algorithms that take the MRI, and put the SPECT on top of it. And then we calculate what we call the anatomical to functional matching. So we want to look at areas like I explained earlier, that are not completely dead, not necrotic. But have low metabolism. those are the areas that we want to take a look at. Can I share my screen? I’m not sure if it’s visual or not.
Bill Gasiamis 34:16
The penumbras right? You can show, so you’re talking about the penumbras. Now before you show anything, are we talking about even in patients that are 10 years post stroke? Could there be penumbras active or able to be rehabilitated?
Dr. Amir Hadanny 34:34
Yes, exactly. That’s the exact thing that we discovered. There’s something that’s called a chronic penumbra. A lot of people know about the acute penumbra that we look in the first couple of hours of the stroke, but we’ve realized that there is a chronic penumbra years after the stroke. And that’s exactly what we’re looking for in the SPECT.
Bill Gasiamis 35:00
Okay, please do feel free to show us some of your images.
Dr. Amir Hadanny 35:07
I’m gonna try and show a case.
Intro 35:10
If you’ve had a stroke, and you’re in recovery, you’ll know what a scary and confusing time it can be, you’re likely to have a lot of questions going through your mind. Like, how long will it take to recover? Will I actually recover? What things should I avoid? In case I make matters worse, and doctors will explain things that obviously, you’ve never had a stroke before, you probably don’t know what questions to ask.
Intro 35:34
If this is you, you may be missing out on doing things that could help speed up your recovery. If you’re finding yourself in that situation, stop worrying, and head to recoveryafterstroke.com where you can download a guide that will help you. It’s called seven questions to ask your doctor about your stroke.
Intro 35:54
These seven questions are the ones Bill wished he’d asked when he was recovering from a stroke, they’ll not only help you better understand your condition, they’ll help you take a more active role in your recovery, head to the website. Now, recovery after stroke.com and download the guide. It’s free.
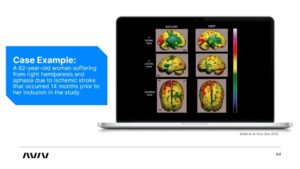
Dr. Amir Hadanny 36:13
So this is a nice example of what we just talked about. So this is a 62 years old woman who suffered a stroke 14 months before coming to us. So a year and two months before that, she suffered a left side stroke an ischemic stroke, meaning her MCA artery was occluded.
Dr. Amir Hadanny 36:39
And because it’s on the left side, and she’s left side dominant, she suffered from right hemiparesis meaning right weakness in the right side, and aphasia, meaning she was unable to speak. So we did the MRI, and we did the SPECT scan. And what you see on the screen right now on the left side is the baseline SPECT.
Dr. Amir Hadanny 37:07
And, again, this is on top of the MRI scan, this is coregistered. And what we’re looking for here is the level of metabolism or level of function. So yellow is the average activity, red is high activity, green is low metabolism, low function. What we found, we found two specific areas that are low function here, what you see here, I don’t know if you can see my mouse, that’s the motor cortex, area of the motor cortex with low metabolism.
Dr. Amir Hadanny 37:44
And here, this is what we call it the Broca’s area, this is where we generate speech from. Both of these areas, are green meaning low metabolism. When we saw this, we said, okay, there is a logic to do the protocol. So we included her in the protocol that we’re going to discuss in a minute, what is the protocol, and after three months of the protocol, this is proposed scan.
Dr. Amir Hadanny 38:17
So we rescanned the same person afterwards with SPECT, and you see here, the green areas, most of it became yellow, most of the motor cortex, and both in the broca, you see some leftover green, but most of it is yellow, and this correlated with significant improvement in her right hand and her right leg movement, and she regained speech.
Dr. Amir Hadanny 38:46
Again, it was not as perfect as she was before the injury, but she was able to talk. And this is 14 months afterwards. I don’t know if everybody knows this. But basically, when we give the prognosis or we predict what’s going to happen for a stroke survivor, somewhere after the three to six months after the injury, their rehabilitation reaches a plateau. So whatever we regained in those three, six months stops. Here, we show that even 14 months afterwards. We still can regain rehabilitation.
Bill Gasiamis 39:37
That’s great news. I’ll tell you why. It’s great news. Firstly, because people get to the plateau. Doctors don’t do a good job of explaining what the plateau is and what it means. And then people leave hospital thinking that that’s it, no more recovery for them.
Bill Gasiamis 39:55
And that’s a big issue when doctors send people home and they feel like there’s no recovery, then lots of things can go get in the way to prove that there isn’t going to be any more recovery with the patient becomes potentially one of the people that proves the doctors, right. And, and that can be sad if that’s the case.
Bill Gasiamis 40:17
But what I love here is that you’ve actually got imaging for the first, one of the first times I imagine where you’re proving that beyond the plateau, there are numbers that can be rehabilitated in the brain, and therefore, restore function that is fantastic to hear. That is such an amazing thing.
Dr. Amir Hadanny 40:42
Exactly. And that’s the key thing. That’s the key. And that’s how you select patient, you literally understood what we’re talking about it, we want to see those chronic pain numbers, prove that they’re there. And if we find them, and we find them in most of our patients, we find them and they correlate with the symptoms, then we should do the hyperbaric oxygen therapy protocol. That’s exactly.
Bill Gasiamis 41:09
That is amazing. That’s so heartwarming. That’s so good to hear and see to actually visually see that. Now, when you first discover this, do you know what you’re discovered? Do people gather behind you and support you to take this to the next level? How does it get? How does it get up to that next level? Because I imagined in 2008, when all this started, do you guys would have been excited, but were you able to get the rest of the community excited.
Dr. Amir Hadanny 41:44
We’re trying I gotta tell you this is this is a working process. This is a process. And you know, I’m, I’m meeting with neurologists and neurosurgeons day in day out, I need I need to give the same talk and show them everything again, and again. Because even though we published, it’s not out there as much as it should. So it’s slowly getting them. We’re doing our best. But still, good one out there.
Bill Gasiamis 42:20
Good work. So just before we go into the actual protocol, I’m wondering about what you’re actually achieving here. So we hear about Neuroplasticity, and a lot of stroke survivors, it’s one of the first things they hear about when they go into a hospital after they’ve had a stroke. And when they go into rehab for the first time, you get the Neuroplasticity speech. And I think that’s an amazing speech.
Bill Gasiamis 42:45
Because, you know, Neuroplasticity can occur. Simply by imagining yourself walking, you can be creating new neural pathways to support the pathways that are no longer there, or pathways that have been lost so that you can when you go back to therapy, as you begin to walk, you’re enhancing the neural pathways that you’ve just imagined in the past.
Bill Gasiamis 43:10
And then you walk, even if you’re in the stirrups, even if you’re holding on to the bars, even if you’re in your cane or whatever you’re doing. And then what you’re doing is creating new neural pathways to to go around, I suppose for lack of a better medical word from me to go around the old ones, which are no longer working right.
The four components of the protocol
Bill Gasiamis 43:32
Now, in this case, are you re igniting old neurological pathways that were there? Are you bringing cells back to life? Are you like, what are you actually doing to the brain when those Penumbra has rehabilitated? How does it work?
Dr. Amir Hadanny 43:57
So there are four components that we have discovered that by doing our protocols that we’re actually doing. So the first one we’re providing energy to reignite I like that tendency use reignite those areas that were not that. So the necrotic areas, you know, after several months, the areas that suffered from damage beyond repair, they’re dead and there are no cell there.
Dr. Amir Hadanny 44:27
There are no cell there. It’s just water. So on those areas, on water, we cannot work. But those areas with the penumbra, those, those are cells that are alive, but are not friends meaning electricity. They have enough energy to survive, but they’re not doing action potentials that actually transmit data.
Dr. Amir Hadanny 44:52
Those are the areas that we reignite with the high level of oxygen. That’s number one. Number two What we found, we have a specific protocol. And again, we’re going to talk about exactly how we do it. But we’re doing something called oxygen fluctuations, meaning that each time the patient goes in the session, we’re doing several minutes with oxygen several minutes without, with oxygen.
Dr. Amir Hadanny 45:27
Without what it does. It’s something we call oxygen fluctuations. So high levels of oxygen normal level of oxygen, high level of oxygen, normal level of oxygen. What it does is it tricks the brain tricks each cell in our brain to think that it’s suffering from stroke, again, that it’s under stress that it has low level of oxygen.
Dr. Amir Hadanny 45:53
The reason we’re doing this is when the brain feels this, it triggers a specific molecule called one Alpha, our toxic induce factor one Alpha, that’s the trigger for brain repair. And that’s, and we have that in the first three months. That’s why we finish up with the plateau. Because the brain secretes that on its own in the first several months.
Dr. Amir Hadanny 46:21
But then it stops, we are able to force the brain to continue to secrete this molecule, this trigger of brain repair, by just by tweaking this high level normal level, retrieving it to continue repairing itself. That’s number two. And this is critical that we’re doing it on a safe level. Because the other way you could have had it if you I guess cause multiple strokes on yourself or choking, but that’s unsafe. By doing it high level to normal.
Dr. Amir Hadanny 46:58
We’re never in the unsafe areas. And we’re still triggering brain repair. That’s number two. Number three effects that we are able to do is we are we have shown we are recruiting stem cell neural stem cells, we’re actually bringing neural stem cells that can build new nerves in the brain areas that were injured, they’re not building it anywhere. They’re just building it, where the injury happened.
Bill Gasiamis 47:29
I like that I’m gonna interrupt there, you said something really important. You said they’re not building anywhere. So you hear a lot about stem cell therapy. And usually they’re infusions or injections, and they’re not targeted, they just go into any particular place. And it seems like they hope for the best.
Bill Gasiamis 47:47
And that was one of the things that I kind of struggled with when I heard about stem cell therapy. Is that how do you know where the stem cells are going to go? How do you get them to go where you want them to go?
Bill Gasiamis 47:57
So what you’re doing here is by by tricking the brain into thinking that it’s hypoxic, because it’s had that increased boost of oxygen, and then you’ve taken it down to normal levels. It’s going oh, my gosh, we got problems right here, we need to create neural stem cells right here right now in that spot.
Dr. Amir Hadanny 48:24
Exactly. Exactly the thing. You know, I couldn’t have upgraded better. I think a lot of people are injecting stem cells in the spine in their veins, I was even part of a study that, you know, we did it intracranial. So people injected stem cells in the brain itself. It doesn’t work.
Dr. Amir Hadanny 48:47
And you know, every decade, we see another study that people try to do it and it doesn’t work. And the reason it doesn’t work, because these are external stem cells that have no reason to, oh, I’m injected here, okay, I’m going to build something, they don’t have the trigger that I mentioned, and they don’t have the infrastructure to stay there and build it. So they’re just being injected, they’re floating around and die.
Dr. Amir Hadanny 49:15
That’s what happened to the stem cells that are being injected in so many clinics, so many areas. So it’s a shame. I mean, it has good logic, but then again, it doesn’t have good logic. And everyday can people think that they solved it? So far, all these external injections do not work.
Dr. Amir Hadanny 49:38
What we’re doing is we’re using our own energies, meaning our own bodies themselves, flowing to where they’re needed. And the fourth component is also the critical part that people are forgetting the infrastructure themselves will survive. If are being supplied with oxygen and blood, they need something to survive it. They’re not just it’s not like a Petri dish that you put them on.
Dr. Amir Hadanny 50:10
And they’re surviving, they they need something to hold on. So the fourth component of our protocol is inducing blood vessels. So we are building new blood vessels that are being formed in those areas. And again, in the areas that need it, it’s not, we don’t get new blood vessels in our hands.
Dr. Amir Hadanny 50:32
It’s just in those areas, we see that. So the stem cells can actually be supported to build new nerve cells. So in medically or scientifically, it’s called angiogenesis, the generation of new blood vessels and neurogenesis, the creation or generation of new nerve cells. Those are the four facts that we’re actually doing.
The discovery of new blood vessels in the brain
Bill Gasiamis 50:59
New blood vessels. Is that a fairly recent discovery? Is it something that’s been recently understood? Because I didn’t realize that we could increase the number of blood vessels in your brain.
Dr. Amir Hadanny 51:15
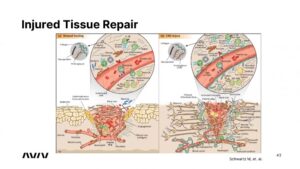
So we know about new blood vessels from the wounds, you know, so we knew that hyperbaric medicine or hyperbaric oxygen therapy induces new blood vessels in those diabetic wounds. And I think that the biggest concept and again, I guess I’m gonna share a very slide here, that’s kind of critical to understand.
Dr. Amir Hadanny 51:40
This is a nice slide from the Weitzman Institute in Israel that was recently published. And what it shows, on the left side is how a wound in our leg or in our hand is healing. And on the right side, is a wound in our brain, which is a stroke.
Dr. Amir Hadanny 52:02
And, you know, when I grew up, and when I got my medical education, people have told me, you cannot repair the brain, nothing can. But we know today in this decade, that is, it’s not true, we can repair the brain. And amazingly, it’s really similar. It’s exactly the same concept. So this comparison is beautiful.
Dr. Amir Hadanny 52:27
So the cells names are different. But it’s exactly the thing things happening here. We need vessels, we need the inflammatory cells, we need new nerve cells coming in, all these processes are occurring, exactly the same in the wound in our hand, and in the wound in our brain.
Dr. Amir Hadanny 52:51
And when we understand this, we can supply those four components that I’ve mentioned. So since we knew that in the wounded leg, we are actually getting new blood vessels. We just tested it out in our brains in our stroke. And we showed that we’re also doing the same thing. In our stroke area, we are creating new blood vessels.
Bill Gasiamis 53:18
I love it. Absolutely love it. So what we’re doing is the good thing about seeing this on a wound on the leg is that we get to see the wound heal, we physically get to see heal and close over, but we can see inside the brain under normal circumstances. So that would be invisible.
Bill Gasiamis 53:36
And I imagine when you guys first discovered this in 2008, you know, the people came to you, they said, Oh, we feel better in the head. Our cognition is different. Our stroke symptoms have eased or changed or become better. And that makes sense that you would go well, okay, that doesn’t mean anything to us.
Bill Gasiamis 53:57
Because we saw the wound heal on the leg or on the arm, but we didn’t visually see anything inside the head. So let’s go through the process of proving that by doing the study. I love the way the whole process has worked. And the way you guys think and the way that it’s got like that.
Bill Gasiamis 54:15
Now, what I also love about it is that visual that slide, it makes a real big difference to me. Because when I’m doing stroke recovery, and I get to see, and I get to go through the process of hearing that I’ve reached the plateau. And then by chance, I’ll learn about the penumbra.
Bill Gasiamis 54:37
And now by chance I’ve learned about the pin numbers that persist that are there beyond the plateau that can still be rehabilitated, and then I get to see the proof, the physical proof of a wound healing on somebody’s arm, which confirms that there are blood vessels occurring for regenerating in that particular wound.
Bill Gasiamis 55:03
And then I get to see the same thing in the brain, you’ve got me convinced I’ve understood the whole path, the whole process to get me to the point where I completely, totally understand how we can restore function in the brain in a spot that’s been previously damaged. That’s fabulous.
Dr. Amir Hadanny 55:22
Perfect, perfect. I, I love that. I reached to the crowd and I and people understand this concept, because it’s not it’s not easy to understand. And, you know, I have physicians and neurologists that it takes time for them to drop. But that’s, that’s what we’re trying. And that’s what we’re trying to convey here. And this is great news, like you said,
Bill Gasiamis 55:47
yeah, it is great news. I think neurologists have a different way of thinking about things, I think very simplistically, right? So I don’t need a lot to be convinced. And sometimes that’s the challenge is with stroke survivors, they don’t need a lot to be convinced.
Bill Gasiamis 56:00
They say, here’s something about hyperbaric oxygen therapy, they go by a tank, they put it in their in their house, because the guy who sold it to them, convinced them very easily or very well, that that’s what they needed. So they went and got it right.
Bill Gasiamis 56:14
Whereas I, I might be that way inclined. But this just makes me feel a lot better about the whole thing, and you’re not selling me anything. And that’s even better. So fun. So that’s awesome work. I just love the work that you guys are doing. So that’s the that’s is that the entire protocol. That’s part of the protocol. Right?
Dr. Amir Hadanny 56:37
So So I guess let’s, let’s go back to our journey. So we started with our assessments, right? We did the cognitive we did the physical, we did the imaging, we correlated symptoms with the imaging, we determine that the patient is eligible and will benefit from this.
Dr. Amir Hadanny 56:56
And then he goes through the program, whether the program includes for the program is three months, 60 sessions, five days a week, two hours a day, inside the chamber. And inside the chamber each time, they need to do our protocol, this same protocol that we use in the randomized control trial, I don’t know about different protocols, I know about this one, this one was able to induce those four components.
Dr. Amir Hadanny 57:25
So we do this 60 times, five days a week, two hours a day, we month. And then in usually, on top of that really determine case by case, if we’re going to add cognitive training or physical training on top of the chamber, maximize the efficacy in the trials, we did not use them. We did not use any physical therapy, any cognitive training, because we just wanted to show the hyperbaric oxygen therapy effect.
Dr. Amir Hadanny 58:02
But obviously, when a patient comes in, outside of a clinical study, I want to give him the maximize the maximum effect. So again, the Chamber then I considered do I want to combine it with physical therapy and cognitive training, and maybe a specific diet if I think it’s going to be beneficial.
Dr. Amir Hadanny 58:22
Do this three months. And at the end of the three months, we’ll repeat everything. So we repeat come to function, we repeat physical function assessment, and we repeat the SPECT scan, there’s no need to repeat the MRI scans because we know about anatomy, we want to see about metabolism.
Dr. Amir Hadanny 58:41
So we repeat the specs and like we saw about the lady we saw earlier, repeated and we want to see if we were able to heal those brains, those areas of chronic pain numbers, exactly that.
Bill Gasiamis 58:59
So a 62 year old person is not restricted by age with regards to being able to generate their own stem cells.
Dr. Amir Hadanny 59:07
Nope. We have actually done an aging study. We’ve got an aging study on people over 6070 and 80 years old. And we have shown that we recruiting the number of stem cells just as much as we do on younger people.
Bill Gasiamis 59:26
Wow, that’s good news, too. Yeah. Because it’s because yeah, because it’s often often suggested that people who are older, probably candidates for stem cell injection therapy or something along those lines because of the fact that they are older and because of the fact that they’re less likely to be able to generate growth hormone and other other factors.
Dr. Amir Hadanny 59:59
There on AIM Well, too, in their normal physiology, as we get older, we don’t have the trigger for repair. But if you’re doing the protocol, you’re forcing their body and their brain to induce those triggers, just like in earlier. So it’s true that normal physiology makes an ageing brain to do less repair, but if forcing it to induce the trigger, it will repair itself. Okay.
Bill Gasiamis 1:00:31
So your, your patient has to commit to a fair routine a fair regimen of treatment, five days a week, two hours a day? Are those two hours in the chamber at the same time? Or are they different times? Or
Dr. Amir Hadanny 1:00:53
usually a think we can accommodate it, we’ve, the patient needs to move it here and there, but usually it’s saying they every day, five days a week, two hours
Bill Gasiamis 1:01:04
solid in the chamber? Alright, okay, where does? Where does your work take place, which part of the world.
Dr. Amir Hadanny 1:01:13
So we started in Israel, that’s where we did all the research. And then we started deploying clinics. So we have a clinic in Dubai, in Asia, then a clinic in the United States in Central Florida. Those are the first two clinics and we’re expanding. Next year for more clinics, we’ll have one in New York City, and more to come in.
Dr. Amir Hadanny 1:01:38
Because the goal is to touch the lives of everyone we can in. We haven’t discussed this, but as you know, stroke is the real pandemic. You know, people learn the word pandemic, past three years, but stroke is the real one. You know, it happens every minute, anywhere in the world.
Dr. Amir Hadanny 1:02:03
And there are so many stroke survivors that people don’t even understand how many. So we want to reach out as much as possible, anywhere we can. And to provide them with the high quality protocol that we know that can help them.
Bill Gasiamis 1:02:23
One in four people, I think the World Health Organization’s says that will experience a stroke in their lifetime, it’s dramatic, and a lot of those people, majority of those people end up with some kind of a disability. And it’s a big challenge. Is that particular protocol that you’re able to facilitate people for Is it expensive? How do people pay for that? Is it reliant on their insurance? How do you go about bringing people on board?
Dr. Amir Hadanny 1:02:56
I think that’s the most painful part, at least for me. Right now, it’s not covered by an insurance. So it’s all out of pocket for the patient. It remains a bit expensive, I would say, for a lot of patients we are I think that’s well, I don’t think I know, this is my My life goal to make it true.
Dr. Amir Hadanny 1:03:22
And that’s why I do my studies. We are planning to do more and more research in order to get it approved, you know, medical in order to get a medication or any procedure approved by insurance. He takes a lot of time and a lot of years to get approved.
Dr. Amir Hadanny 1:03:42
We are doing this we are in the process, but it will take many more years until we get we get that approval and signature here the insurance is going to cover it. But that’s what are we doing? That’s what I’m doing. But we’re not voting for the time being. It’s not covered and it’s out of pocket for the patients.
Bill Gasiamis 1:04:03
Yeah. The people who are deploying the clinics in other countries, and then deploying them on the on your behalf. Are they other colleagues that are involved in the research? How does another clinic get set up? Of course, we don’t need another whole process, but like how does somebody get
Bill Gasiamis 1:04:21
a new location gets selected, and then a new clinic established?
Dr. Amir Hadanny 1:04:25
So I’m part of the team of the company that doing those clinics. I’m the chief researcher, and the head of the medical operations. So when we set up a new clinic, it’s being built from ground and we select our physician, I trained them.
Dr. Amir Hadanny 1:04:48
I trained him personally on the protocols and how it’s done and I usually spend time with the physicians in the clinic for several months in order to make Make sure we get high quality protocols and we select the right patients, we do the right treatments, because you know, I am as strict as possible and the quality that we want to deliver. So I personally oversee everything.
Bill Gasiamis 1:05:18
Now, I know I’m a stroke survivor. So it’s my favorite topic to discuss helping stroke survivors. So I love that workbook when I’m on the website at aviv-clinics.com. And I’ll have the links for the website in the show notes.
Bill Gasiamis 1:05:34
I’m noticing there’s a whole bunch of other things that oxygen therapy has helped people with, including PTSD, including people that are 82 years old, helping them to run marathons, including a whole bunch of other things. But the PTSD one really struck me.
Other field of study of Dr. Amir Hadanny
Bill Gasiamis 1:05:56
So again, is that something that was discovered by accident through these types of protocols, and that has expanded into other areas of research? How did these things come about?
Dr. Amir Hadanny 1:06:10
Awesome question. So my other passion as a neurosurgeon, except stroke is traumatic brain injury, which is a very, you know, very, I guess, political or discussed matter. You can get traumatic brain injury from sports, NFL, rugby, or you can get it in the military, from different accidents, different explosion, different events, or even a regular motor vehicle accident. So I treated a lot of traumatic brain injury patients.
Dr. Amir Hadanny 1:06:47
So we saw a lot of them are suffering from different disabilities after the treatment, whether it’s a mild concussion or whether it’s a severe injury. And again, during my residency, after the stroke study was completed, when we understood about chronic penumbra, as we said, we need to understand what’s going on with traumatic brain injury.
Dr. Amir Hadanny 1:07:11
And we basically found the same thing. If you had a traumatic brain injury several years back, we want to see if we find penumbras, we want to see if we find penumbra in your brain, and if so, do they correlate with those symptoms? And if so we can treat them. So we’ve done this, again, several randomized clinical trials, both in adults and in pediatrics.
Dr. Amir Hadanny 1:07:40
And out of that, just to go back to your question. Some of TBI patients suffer from PTSD. And then we got the reports from several of our patients that their PTSD is changing. And I gotta tell you in the first couple of session, it can actually deteriorate, we found out that in first two or three weeks, people are re experiencing things.
Dr. Amir Hadanny 1:08:11
And we had to help them go through those several weeks. And afterwards, they go back into sessions, and they come out differently. And when we realize we can actually affect PTSD, we started a randomized control trials for PTSD. One of them is still running right now in Israel.
Dr. Amir Hadanny 1:08:35
And we’re seeing some nice results, we’re going to publish them, we did the first study on it. Now, we’re reconfirming the evidence we’ve got. So very exciting. And it all comes down to understanding what’s going on in the brain. Doing patient selection based on what we see on brain imaging and the correlation to symptoms.
Dr. Amir Hadanny 1:09:02
If you don’t have it, not going to do anything, you have to actually see the brain and select your patient based on that, regardless of the pathology.
Bill Gasiamis 1:09:14
Dr. Haddany this is a really amazing interview. Thank you so much. I really appreciate it. The information that you shared, I think offers hope, more than anything to the people who are listening and watching. If you’re listening, you definitely need to go to the shownotes. So you can see the slides that we were speaking about.
Bill Gasiamis 1:09:33
And if you’re on YouTube, hopefully you’ve actually seen the slides that we’re talking about because I think they really are picture paints 1000 words, as far as I’m concerned. So they’re really important. I’ll plaster them everywhere and make sure that you guys get to see them.
Bill Gasiamis 1:09:51
I just wish you guys every success in the work that you’re doing. I think it is going to be unbelievably successful. I hope that you guys have clinics all over the world. And I’m looking forward to the first clinic opening in Australia, I might go and visit it myself.
Dr. Amir Hadanny 1:10:11
Thank you so much. Thank you. I’m really hoping to get as much as possible done, and get it all approved and help as many stroke survivors because really, this is a life goal of mine. And we hope to succeed and actually affect people’s life. Do good is our motto.
Bill Gasiamis 1:10:33
Dr. Haddany, thank you for being on the podcast.
Dr. Amir Hadanny 1:10:36
Thank you so much.
Bill Gasiamis 1:10:38
Thank you for joining us on today’s episode, I hope you got a lot out of this particular interview, I certainly did the hope that the work that Dr. Madani is doing and that offers stroke survivors is really truly amazing and groundbreaking.
Bill Gasiamis 1:10:56
They’re talking about things that I’ve never heard before, that is very seldom spoken about these long term spots in the brain that are still kind of low in energy and need some assistance to get back to working in some way shape or form.
Bill Gasiamis 1:11:14
And then hopefully restoring some potentially lost function to stroke survivors, even after many, many years beyond stroke. So the fact that the imaging has gotten to the point where it is enabling people to find these new places these new power numbers that can be rehabilitated is truly amazing, I was really excited to hear the information that Dr. Haddany shared.
Bill Gasiamis 1:11:48
Now if you’d like to learn more about my guests, including links to their social media and other pages, to download a full transcript of the entire interview, please go to recoveryafterstroke.com/episodes. If you would like to try the course five foods to avoid after stroke, go to recoveryafterstroke.com/courses. If you would like to support this podcast, the best way to do it is to leave a five star review.
Bill Gasiamis 1:12:17
This is a really important thing that I would ask anyone listening who has a moment and can can do please do leave the show review because it’s going to make it easier for other stroke survivors like you who needed this type of information, find it easier, and that’s going to make it better on the path to recovery for them. For those who have already left the review. Thank you so much. I really appreciate it.
Bill Gasiamis 1:12:42
It does make a huge difference to how we go through this recovery process. If you leave a few words on iTunes, and Spotify, they’re the best places. Also on YouTube, you can leave a comment below, ask me a question. I’ll respond. I’ll answer your questions. Give the show a thumbs up subscribe.
Bill Gasiamis 1:13:03
Any interaction with any of these podcast episodes just makes a massive difference to the way the search engines make it so that other people can find the show. Now, if you’re a stroke survivor with a story to share, come and join me on the show. The interviews are not scripted, you do not have to plan for them.
Bill Gasiamis 1:13:24
All you need to do is be a stroke survivor. Here’s somebody who is a stroke who is a stroke survivor, and be one of the amazing people like Dr. Haddany who do work that improves the lives of stroke survivors. It doesn’t matter whether you’re a doctor or an allied health professional.
Bill Gasiamis 1:13:45
Anyone at all, who’s in that space is welcome to join us on the show. Go to recoveryafterstroke.com/contact fill out the contact form. As soon as I receive it. I will respond with more details on how you can choose a time that works for us both to meet over zoom. Thank you for being here and listening. I really appreciate you see you on the next episode.
Intro 1:14:10
Importantly, we present many podcasts designed to give you an insight and understanding into the experiences of other individuals.
Intro 1:14:17
The opinions and treatment protocols discussed during any podcast are the individual’s own experience and we do not necessarily share the same opinion nor do we recommend any treatment protocol discussed all content on this website at any linked blog podcast or video material control this website or content is created and produced for informational purposes only and is largely based on the personal experience of Bill Gasiamis the content is intended to complement your medical treatment and support healing.
Intro 1:14:44
It is not intended to be a substitute for professional medical advice and should not be relied on as health advice. The information is general and may not be suitable for your personal injuries, circumstances or health objectives. Do not use our content as a standalone resource to diagnose treat cure. prevent any disease for therapeutic purposes or as a substitute for the advice of a health professional.
Intro 1:15:05
Never delay seeking advice or disregard the advice of a medical professional, your doctor or your rehabilitation program based on our content. If you have any questions or concerns about your health or medical condition, please seek guidance from a doctor or other medical professional.
Intro 1:15:19
If you are experiencing a health emergency or think you might be, call 000 if in Australia or your local emergency number immediately for emergency assistance or go to the nearest hospital emergency department. Medical information changes constantly.
Intro 1:15:31
While we aim to provide current quality information in our content. We did not provide any guarantees and assume no legal liability or responsibility for the accuracy, currency or completeness of the content. If you choose to rely on any information within our content, you do so solely at your own risk. We are careful with links we provide however third party links from our website are followed at your own risk and we are not responsible for any information you find there.