Does GABA Actually Help With Sleep? What the Research Says for Brain Injury Recovery

Someone in our community recently asked me about GABA for sleep. They’d seen it recommended online, understood that sleep was critical for their recovery, and wanted to know whether the supplement was worth exploring or just noise.
It’s a genuinely good question. And it deserves a proper answer.
In this post, I’m going to walk you through what GABA is, what the clinical research actually shows about its effect on sleep, why the blood-brain barrier debate matters (and why it might not derail the whole argument), and what the evidence says about the relationship between sleep and brain recovery. By the end, you’ll have enough to have an informed conversation with your medical team.
I’m not a doctor. I’m a three-time haemorrhagic stroke survivor who has spent years researching the science of brain recovery and interviewing hundreds of clinicians and survivors on the Recovery After Stroke podcast. What I offer is a careful read of the evidence, not a clinical prescription.
What Is GABA and Why Does It Matter for Sleep?

GABA (gamma-aminobutyric acid) is the brain’s primary inhibitory neurotransmitter. If your nervous system were a car, GABA is the brake pedal. It reduces neuronal excitability, quiets cortical arousal, suppresses the brain’s primary arousal centre (the locus coeruleus), and modulates the HPA axis, the stress-response system that drives cortisol.
Most sedative medications work by amplifying GABA activity. Benzodiazepines, for instance, bind to GABA-A receptors to increase chloride channel opening, producing their calming effect. GABA isn’t doing something unusual here – it’s doing something fundamental.
The question with supplemental oral GABA is more specific: Does taking GABA as a capsule or powder actually produce meaningful neurological effects?
What Does the Research Show?

Finding 1 — Oral GABA Reduces Sleep Latency (and EEG Can Measure It)
A 2015 clinical trial published in the Journal of Nutritional Science and Vitaminology by Yamatsu and colleagues used EEG measurement, actual brainwave monitoring, rather than self-reported sleep questionnaires. One hundred milligrams of oral GABA shortened sleep latency (time to fall asleep) by 5.3 minutes compared to placebo.
That might sound modest. But for someone lying awake for 30–40 minutes each night, it’s a meaningful shift. Crucially, this was objective neurophysiological data, not a survey response. (PMID: 26052150)
Finding 2 — A 90-Day RCT Showed Improved Sleep Efficiency and Mood
A 2024 randomised double-blind placebo-controlled trial published in the Journal of Dietary Supplements (Guimarães et al.) gave 200 mg of GABA daily for 90 days to sedentary overweight women also undergoing an exercise program. The GABA group showed significantly improved Pittsburgh Sleep Quality Index (PSQI) scores, significantly reduced depression scores, and improved heart rate variability, a marker of parasympathetic nervous system activity.
The HRV finding is particularly interesting. It suggests GABA may be doing something broader than simply reducing sleep latency – it appears to support the overall physiological state that makes rest restorative. (PMID: 38321713)
Finding 3 — But a High-Dose RCT Found No Effect
Here’s where intellectual honesty matters. A 2023 Dutch RCT (de Bie et al.) published in the American Journal of Clinical Nutrition gave participants 500 mg of GABA three times daily, 1,500 mg/day total, and found no significant effect on self-reported sleep quality. Fasting plasma GABA wasn’t significantly elevated either, raising real bioavailability questions at that dose.
This isn’t a reason to dismiss GABA entirely. It is a reason to pay attention to the dose. The evidence base supports 100–300 mg, not 1,500 mg. Higher is not better, and the non-linear dose response is clinically important. (PMID: 37495019)
The Blood-Brain Barrier Debate — and Why the Gut May Be the Point
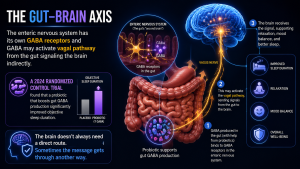
The most common objection to oral GABA supplementation is this: GABA is a zwitterion at physiological pH, meaning it has low lipophilicity and poor predicted ability to cross the blood-brain barrier via passive diffusion. So if it can’t get into the brain directly, how does it produce neurological effects?
The emerging explanation involves the gut-brain axis.
The enteric nervous system, your gut’s own neural network, has GABA receptors. When oral GABA activates these enteric receptors, it can signal the brain via vagal afferents without needing to cross the BBB at all. Think of it as a side door rather than the front entrance.
Supporting this: a 2024 RCT (Li et al.) found that a probiotic strain engineered to increase gut GABA production significantly improved objective sleep duration as measured by wearable devices, alongside reduced cortisol and suppressed HPA axis activity. The mechanism wasn’t direct CNS access – it was gut-brain signalling. (PMID: 39385735)
The BBB debate doesn’t negate the clinical effect. It changes how we understand the mechanism.
Why Sleep Is Not Optional in Brain Recovery
This is the part that I think gets underweighted in recovery conversations — and the research is unambiguous.
A 2026 large retrospective cohort study (Muhtar et al., Sleep Medicine) matched over 35,000 stroke patients and found that post-stroke insomnia was associated with a 29% higher risk of post-stroke cognitive impairment and a 30% higher risk of all-cause dementia. The association with Alzheimer’s disease was also significant. (PMID: 41924789)
A 2024 observational study from Monash University and Alfred Health (Smith et al.) found that in stroke rehabilitation patients, poor sleep quality was significantly associated with higher fatigue severity and lower salivary BDNF gene expression. BDNF (brain-derived neurotrophic factor) is one of the primary molecular drivers of neuroplasticity. Less BDNF means a less receptive environment for the neurological rewiring that rehab is trying to build. (PMID: 38802847)
And then there’s the glymphatic system: the brain’s waste-clearance mechanism that is most active during deep sleep. Poor sleep means reduced clearance of metabolic byproducts, including proteins associated with neurodegeneration. This is not a theoretical risk. It is an active, ongoing process.
Sleep is not passive recovery. It is one of the primary mechanisms of recovery.
What to Do With This Information
Here are three practical steps if you’re exploring GABA for sleep:
1. Measure your sleep baseline first.
Use the Pittsburgh Sleep Quality Index (freely available online) before you make any changes. Understanding whether you’re struggling with latency, duration, or quality will determine what you actually need to address.
2. If you trial GABA, choose the right form and dose.
Look for PharmaGABA — naturally fermented GABA, derived from Lactobacillus hilgardii, which has the strongest clinical evidence base. A dose of 100–300 mg taken 30–60 minutes before bed is consistent with the positive studies. Avoid very high doses; the null result at 1,500 mg/day is important context.
Important drug interaction note: If you are taking benzodiazepines, anticonvulsants (gabapentin, pregabalin, valproate), or any other GABAergic medication, discuss GABA supplementation with your prescriber before adding it. The additive sedative effect is a real risk. The same applies if you drink alcohol regularly.
3. Don’t skip the foundation.
Sleep hygiene interventions, consistent sleep and wake times, a dark and cool room, and no screens in the 60 minutes before bed, are consistently among the highest-leverage sleep interventions in the literature. GABA may provide a genuine incremental benefit. But it cannot compensate for a fundamentally disrupted sleep environment.
The Bottom Line
The evidence for GABA and sleep is more substantive than I expected when I started researching it. The EEG data is real. The 90-day RCT showed meaningful clinical outcomes. The gut-brain axis mechanism is biologically plausible and now has direct RCT support. And the consequences of poor sleep in neurological recovery are not trivial – they are quantifiable, significant, and, to a degree, addressable.
GABA is not a guaranteed fix. Individual responses vary. The research is not yet definitive at the level of large multi-centre trials in neurological populations. But as one tool in a comprehensive approach to sleep quality alongside good sleep hygiene, appropriate medical support, and consistent rehabilitation, the case for cautious exploration is reasonable.
The next step is a conversation with your neurologist, GP, or rehab physician. Take the research with you if it’s useful.
Research References
All studies cited in this post are retrievable via PubMed:
- Yamatsu et al. — GABA sleep latency EEG clinical trial (2015) — PMID: 26052150
- Guimarães et al. — GABA 200mg RCT, sleep efficiency + mood (2024) — PMID: 38321713
- de Bie et al. — GABA high-dose RCT, null sleep result (2023) — PMID: 37495019
- Li et al. — Gut-brain GABA axis and sleep RCT (2024) — PMID: 39385735
- Muhtar et al. — Post-stroke insomnia and cognitive decline cohort (2026) — PMID: 41924789
- Smith et al. — Sleep, BDNF, and fatigue in stroke rehabilitation (2024) — PMID: 38802847
This post is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional before making changes to your supplementation or treatment plan.
If you or someone you care about is recovering from a stroke, brain injury, or any neurological condition, the Recovery After Stroke podcast and this blog exist for you. Subscribe on YouTube @BillGasiamis, or visit Recovery After Stroke to find episodes, resources, and community.