EECP Therapy and Stroke Recovery: Can a Cardiac Treatment Help Grow New Blood Vessels?
When I first heard about EECP therapy in the context of stroke recovery, I was skeptical. It’s a cardiac device approved in Australia for stable angina and congestive heart failure. Stroke is not on the label. So why are we talking about it on a stroke recovery podcast?
Because the mechanism is fascinating. And the research, while still emerging, is pointing somewhere worth paying attention to.
In this episode, I sat down with Jack Clifford, a heart disease patient who discovered EECP therapy and began exploring its potential beyond its approved indications. What started as a cardiac conversation quickly became one of the most scientifically interesting discussions I’ve had on the show.
What Is EECP Therapy?
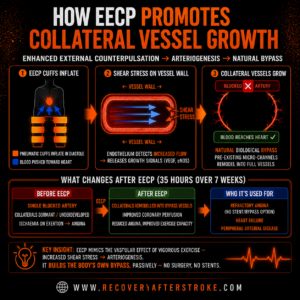
EECP stands for Enhanced External Counterpulsation. The treatment involves a set of pneumatic cuffs fitted around the calves, thighs, and buttocks. These cuffs inflate and deflate in precise synchrony with the heartbeat, inflating during the heart’s resting phase (diastole) to push blood back toward the heart, and deflating just before the heart contracts.
The result is an increase in blood flow and a specific type of fluid shear stress on blood vessel walls. It’s that shear stress that makes things interesting.
The Biology: Arteriogenesis and Angiogenesis
To understand why EECP therapy might be relevant to stroke survivors, you need to understand two terms: angiogenesis and arteriogenesis.
Angiogenesis is the sprouting of entirely new capillary vessels — the body builds small blood channels where none existed before. Arteriogenesis is different: it’s the remodelling of pre-existing, dormant collateral vessels into functional bypass channels. Think of it like upgrading a dirt track into a highway. The track was always there; the body just wasn’t using it.
When blood flow is obstructed, whether by a blocked coronary artery or a stroke, the body can, under the right conditions, activate these collateral pathways. The shear stress produced by EECP therapy appears to be one of the triggers that stimulate arteriogenesis. By generating repeated waves of increased blood flow, the treatment creates the mechanical signal that tells blood vessel walls to grow and remodel.
This is why cardiac researchers originally developed EECP for heart patients. But it raises a legitimate scientific question: could the same mechanism support blood flow recovery in the brain after stroke?
What Does the Research Say?
A 2026 meta-analysis published in the QJM: An International Journal of Medicine examined 15 randomized controlled trials involving 506 participants, looking specifically at EECP’s effects on functional outcomes in stroke patients. The results showed statistically significant improvements, with EECP outperforming control conditions on standard functional recovery measures.
This is preliminary evidence, not a settled clinical consensus. The studies are relatively small, the methodology varies across trials, and EECP remains off-label for stroke in Australia. But for a therapy with a well-understood safety profile and an existing approval framework, 15 studies and 506 participants is not nothing. It’s enough to warrant serious discussion.
What I Discussed with Jack Clifford
Jack came to EECP as a patient, not a researcher. His experience with heart disease led him to explore the therapy, and he’s spent considerable time understanding the evidence base and connecting with practitioners. He’s not a clinician, and neither am I, but what we can do together is examine what the research actually says, what the mechanism actually is, and what questions remain unanswered.
In our conversation, we discussed:
- How Jack first encountered EECP therapy and what led him to investigate it further
- The difference between approved and off-label use, and why that distinction matters
- What the shear stress mechanism actually looks like in practice
- The existing network of EECP practitioners and how stroke survivors might access the therapy
- The questions both of us still have about where the research needs to go
Important Disclaimers
| ⚠️ EECP therapy is approved in Australia by the TGA for stable angina pectoris and congestive heart failure (ARTG Entry 376470). Stroke is NOT an approved indication. This article and podcast episode are not medical advice. Speak with your treating physician before pursuing any treatment. |
This episode is not medical advice. It is a conversation about an area of emerging research that I find scientifically credible and worth understanding. The goal is to help you ask better questions, not to tell you what treatment to pursue.
Where to Learn More
- ecplocator.com a directory of EECP therapy providers
- eecpbook.com is a dedicated resource on the treatment and its evidence base
- recoveryafterstroke.com for stroke survivors looking for a broader community
Research cited: Zhao et al. (2026). Enhanced external counterpulsation for ischaemic stroke: a systematic review and meta-analysis. QJM: An International Journal of Medicine. DOI: 10.1093/qjmed/hcag010.
Therapy and Stroke Recovery: Can a Cardiac Treatment Help Grow New Blood Vessels?
Bill Gasiamis sits down with Jack Clifford to explore EECP therapy, a TGA-approved cardiac treatment that may stimulate the growth of new blood vessels. Together, they examine the emerging research on angiogenesis, arteriogenesis, and whether this off-label approach holds promise for stroke survivors seeking to improve blood flow to the brain.
Highlights:
00:00 Introduction – EECP Therapy
06:06 Recognizing Health Issues and Seeking Help
09:50 Hospital Experience and Heart Health
12:12 Decisions Against Medical Advice
16:28 Exploring Alternative Treatments
18:06 Understanding Enhanced External Counter Pulsation (EECP)
21:58 The Mechanism of EECP
27:03 Personal Transformation Through EECP
30:29 Lifestyle Changes and Holistic Health
34:35 The Impact of Stress on Health
38:30 The Journey of Writing a Book
43:29 The Role of EECP in Heart Health
48:21 Raising Awareness for EECP Therapy
56:05 Exploring the Future of EECP Therapy
Transcript:
Introduction – EECP Therapy
Jack Clifford (00:00)
Mine was really severe. 100 % blocked in my widow maker, the left anterior descending. I’m 95 in my left coronary artery and in my right main, I am 80%. And I’m still that way today, but I can run a sub seven mile.
Bill Gasiamis (00:16)
Welcome to the Recovery After Stroke podcast. I am your host, Bill Gassiamus. Before we get into today’s interview, I need to share something important.
The topic we’re exploring today involves a medical device called an EACP, Enhanced External Counterpulsation Machine. In Australia, EACP is registered with the Therapeutic Goods Administration for the treatment of stable angina and congestive heart failure. It is not approved for stroke. What we are discussing today is emerging off-label research, not a treatment recommendation.
Everything in this episode is for informational purposes only. This is not medical advice. Please speak with your treating physician before pursuing any treatment, therapy or intervention discussed here. With that said, let’s talk about something that genuinely fascinated me when I started reading the research. Your body has the capacity to grow new blood vessels, not just small capillaries, but to remodel dormant pre-existing channels into
functional bypass routes. Scientists call this arteriogenesis. There’s also angiogenesis, the sprouting of entirely new Both processes matter deeply for stroke because stroke is fundamentally a blood flow problem.
Now here’s where it gets interesting. A cardiac therapy developed for heart patients, not stroke patients, trigger exactly this kind of vascular remodeling. And in 2026, a meta-analysis published in the QJM across 15 randomized controlled trials and 506 participants found that EECP
produced statistically significant improvements in functional outcomes for ischemic stroke patients. Now, that’s not proof. That’s not a green light to go and get an EECP, but it is worth a serious conversation. My guest today is Jack Clifford. Jack is a heart disease patient who discovered EECP therapy while managing his own cardiac condition and who has since spent considerable time investigating its potential.
beyond cardiac care. I should tell you, I was skeptical going into this conversation, but I’ve learned that skepticism without curiosity isn’t really skepticism. It’s just closed mindedness. So I read the research and then I sat down with Jack. So if you find this episode valuable, I’d love for you to grab a copy of my book,
The unexpected way that a stroke became the best thing that happened at recoveryafterstroke.com/book. And if you want to support the show, you can join Patreon at patreon.com/recoveryafterstroke. And I want to thank everyone who is supporting me on Patreon, especially the people that have been around for a long time and the people who have just recently signed up. I very much appreciate it. And now here’s my conversation with Jack Clifford.
Bill Gasiamis (03:19)
Welcome to the podcast.
Jack Clifford (03:22)
Thanks, Bill. Great to be here.
Bill Gasiamis (03:24)
Let’s give the listeners a bit of a background understanding of why you’re on the podcast. You’re not a stroke survivor, but we have something in common as ⁓ somebody who has been unwell before myself and you in the past. Tell me a little bit about your journey to the podcast So we just kind of give people an understanding as to how it is that somebody who’s not a stroke survivor.
Jack Clifford (03:34)
We do.
Bill Gasiamis (03:51)
how we ended up chatting together?
Jack Clifford (03:54)
Yeah, absolutely. So the quick version here is ⁓ I was on the brink five years ago of having ⁓ unsentable emergency triple bypass surgery. And ⁓ I chose a different path, which we’ll get to. ⁓ But you you have some level of placking if you have a stroke, typically, depends on the stroke, but that’s typically the case. And in my case, I had placking in my coronary arteries.
So it resulted in heart disease.
Mine was really severe. 100 % blocked in my widow maker, the left anterior descending. ⁓ I’m 95 in my ⁓ left coronary artery and in my right main, I am 80%. And I’m still that way today, but I can run a sub seven mile.
I can do some things that a guy that’s as blocked up as that should not theoretically be able to do. ⁓
Bill Gasiamis (04:49)
All right.
Tell me about life before the injury. What kind of work did you do? How did you go about life? What was generally a day like for you?
Jack Clifford (04:59)
Yeah. So I’m retired military guy. Um, so, you know, been in the military most of my life, um, retired about 10 years ago, a little over that. And, um, so I’ve always been a pretty fit guy. It wasn’t, you know, it wasn’t a fitness issue per se. Um, and, uh, I, I, I had kind of lost some of my self care because my wife had been going through some real significant medical issues that really required my full attention for quite a while.
And because of that, really stopped taking care of myself in the ways I had in the past for about 10 years. And when we had just moved to Florida, I started trying to take care of myself again. And that’s when I discovered all these problems.
Bill Gasiamis (05:44)
So
what does not taking care of yourself look like though?
Jack Clifford (05:47)
Gotta be in a couch potato and being on my computer way too much research and for ⁓ trying to help my wife get better and hold down a job at the same time and raise a family and all these other things that took the priority off of me in that sense that one should be taking care of themselves, meaning exercising, meaning eating the right foods, so on and
Recognizing Health Issues and Seeking Help
Bill Gasiamis (06:09)
You know, caregivers tend to die before the person they’re caring for much more often. And it’s cause of that reason, right? Because time is really taken up by especially full-time caregiving with somebody’s in the house and they need caregiving. need care. The caregiver tends to neglect themselves in every way, shape and form and tends to ⁓ make it about the other person. And then the other person.
Jack Clifford (06:14)
I’ve seen that and heard about it.
Yeah.
Mm-hmm.
Bill Gasiamis (06:39)
seems to be doing okay, but the caregiver is struggling and doesn’t ask for help and doesn’t go and doesn’t go and get looked after. And then things tend to catch up with them and they become the ⁓ sickest person in that relationship.
Jack Clifford (06:55)
It’s
like that whole put your oxygen mask on first on the airplane type thing, right? Like, you know, we can’t we can’t give what we don’t have to give
Bill Gasiamis (07:01)
Uh-huh.
Yeah.
So you, did you notice, did you notice the steady decline in your health? Did you kind of go, I’m not feeling right. I’m a feel a bit sluggish like 10 years down the track, or did it just creep up on you? then you got to this point.
Jack Clifford (07:15)
It
really crept, it really crept. I, you know, like I had initially exercise induced angina, but it wasn’t much exercise that induced the angina. And then it very quickly progressed to trying to walk and getting out of breath and, know, at very basic walking speeds, just moderately paced, you know, anything anybody would do out in your neighborhood. ⁓
Bill Gasiamis (07:39)
Did you know that you
had an angina?
Jack Clifford (07:41)
I did, yeah. I didn’t have a big heart attack episode like some people have. I’m 100 % blocked. There’s no heart attack to happen, right? Because the stuff is, I’m so blocked that it’s just a pure blood flow issue. A lot of people don’t understand that that 50 % blockage is a huge risk for a heart attack because you’re gonna burst a plaque and then go from 50 % to 100 % like that. But you know about collaterals.
And if you have collaterals in place, the blood’s not getting flowing this way, you’re gonna recruit some lead oval collaterals to be able to just get by with your activities of day living. But if you don’t push yourself, you don’t know that you don’t have enough blood flow to do these other things.
Bill Gasiamis (08:22)
Okay, so you got to the point where you were so unwell as far as the blood vessels around your heart were so unwell, they were so blocked that angina led to another escalation or something happened that got you to the point where you realized, okay, things are not good. Now, tell me what angina is exactly and what it’s like to have it. How do you experience it?
Jack Clifford (08:39)
Yeah.
yeah, yeah.
I’d love to talk about that. Bill. at its most basic, it’s a supply demand mismatch. So, you know, the blood flow that’s supplying your heart ⁓ is adequate for X, Y, or Z activities of daily living. You know, walking around the house, doing the dishes, you might have enough blood flow for that, but you don’t have enough blood flow to go run a mile or even walk potentially, you know, or
Hospital Experience and Heart Health
but it’s all about supply demand mismatch. And that’s about just the size of the pipes, you know, if they’re clogged up, how clogged up are they? And, know, ⁓ that’s, really it. So, and what it feels like is it’s scary because it feels like a heart attack. all like, what does a heart attack feel like? Well, there’s a thousand different sort of, ⁓ descriptions of it. ⁓ you know, radiating down your arm or nausea or something in your back, but.
you know, if it’s right over your heart, it’s unmistakable. And that’s at least my presentation of angina. And I think it was a pretty typical one is, you know, I have this weird kind of deep pain. initially, when I, when I started, you know, run, trying to run and got it, I thought, ⁓ you know, I just pulled a chest muscle weirdly over my heart. You know, I’ll stop and let’s see if it goes away. I come back, you know, no, same thing. Okay. Still not better. Let’s do it again. Another couple of days later, so on and so forth. I was just kidding myself, but
I didn’t know anything about the horror at that point. hadn’t had to research all this stuff and do all the deep dive.
Bill Gasiamis (10:16)
That’s the same crazy logic
that stroke survivors put to, I’m feeling weird. I’m dizzy. I’m going to go and lie down. I’m going to rest. It’ll be better later. ⁓ I’m too busy. I’ve got to go to work. ⁓ I’ve even had stroke survivors where somebody’s telling them you maybe you’re having a stroke, you know, just tongue in cheek and they’re like, yeah, no, probably not. ⁓ it’s the same crazy logic that we say about things that are unfamiliar to us that we cannot potentially.
Jack Clifford (10:25)
Mm-hmm.
Mm-hmm.
Yeah. Yeah.
Bill Gasiamis (10:46)
link to something so serious because we have no knowledge, we’re ignorant, right?
Jack Clifford (10:47)
Yeah.
Well, yeah, I think that’s really part of the key there is like most times with something as sudden as what you’re talking about or what I’m talking about in my instance, because it was pretty, pretty sudden, you know, weeks and months. ⁓ We went from being these, you know, healthy people that felt like we were on top of the world to all of a sudden not. you you didn’t have a frame for what not looked like. ⁓
Bill Gasiamis (11:14)
Exactly.
Yeah. That’s such an important comment. We don’t have the frame for what not healthy looks like and therefore you don’t know what you don’t know. So you don’t take any action. You just brush it off. Okay. I hear you. All right. We got to the bottom of the stupidity behind a lot of my decisions as well to avoid going to hospital for a week, et cetera, the first time. ⁓ So you end up
Jack Clifford (11:24)
Exactly.
That’s it.
Bill Gasiamis (11:43)
being really unwell on this particular date. Kind of what is that day like? Explain us.
Jack Clifford (11:46)
Yeah. Yeah.
Decisions Against Medical Advice
So I got tight. I, I, I’ve been a biohacker for a while. So that’s probably the only reason I’m here talking to you because I went off the beaten path really far off the beaten path to get to the place where I know what I know and I have to share what I have to share. ⁓ because I’ve been trying to help my wife get better for some significant issues, including a really bad traumatic brain injury.
And some other things and doctors didn’t have the answers for those so we had to we had to kind of biohack our way out of some things I was comfortable back. I’m saying that to say my wife got me a Chili pad for my bed because you know been trying to biohack sleep for a while and the colder environments to sleep are you know better to some degree at least in theory ⁓ and so Yeah, correct
Bill Gasiamis (12:32)
Chili meaning cold, not spicy.
Jack Clifford (12:37)
Yeah, correct. A chili pad as in the cold. So it’s a device that just, you know, cools your bed off. And so I crank that down to 55. She got it for me for Christmas. So Christmas day Eve, I’m like hopping into bed, like I’m going to sleep really well tonight, you know, and I woke up at four AM like, Oh, you know, I thought that was the big one because it felt that way. I a dead sleep woke me up with, with intense chest pain.
And I knew something was going on, you but I was kidding myself. I hadn’t talked to family about it. You know, I hadn’t shared anything about what was going on with anybody. So at this point I’m like, oh my goodness, you know, and I could be dying and have not had, you know, just been an idiot the whole time. So I rushed to the hospital and I didn’t have a heart attack. I just made it so cold that I made my heart work and that supply demand mismatch was happening all night long in my sleep.
Bill Gasiamis (13:15)
Mm-hmm.
Jack Clifford (13:31)
And so it got to this, you know, a giant, creeps up, you know, it’s like, can feel it. And then if you push it, you’re like, can really feel it. Well, you know, I woke up out of a dead sleep going from not feeling it when I went to sleep to, to feeling it to the extreme when I woke up. Um, but that’s when they gave me the, uh, the, uh, nuclear stress test with a treadmill test, right in the hospital. And it was, it was really bad. They can’t quantify your blockages with that, but they can tell you that, you know, you’re
You’re kind of screwed. And I was like really screwed. Like it was 47, but they said I was one of the worst I’d ever seen. ⁓ yeah. So I had all weekend to think about it, you know, cause I was a Friday, fortunately, and they could, they weren’t going to do the heart catheterization until Monday and the doc, you know, I was signing consent forms for them to do bypass surgery and it was pretty clear that the odds of it getting stented was not really good, but that’s what you hope for. Right. And most people are like, we’ll just get a step.
once then in you’re fine. And ⁓ in my case, it wasn’t looking likely. And my mother had had bypass surgery five years before that. And I watched her cognition after the bypass surgery just declined to the point where she’s in memory care now. And she had gone from being this vibrant book author of multiple books and you know, she was a hypnotherapist and she’s helped a lot of people in her life, done a lot of amazing things, but ⁓ she never.
she never really came out of the bypass surgery as her whole self and pretty quickly was just completely not herself at all. ⁓ So I wasn’t ready to come back. Now she’s 76.
Bill Gasiamis (15:03)
How old? How old’s your mom?
Yeah. I know with people that are older, ⁓ heart surgery can lead to cognitive decline and there is a link there. There is a number of it’s well researched. It’s a risk. ⁓ not one that you’re probably aware of and that they talk about much, but it definitely is a thing. so, okay. You’re, you’re you go to the hospital. They realize, ⁓ the
Jack Clifford (15:15)
Mm-hmm.
Bill Gasiamis (15:37)
charts are not looking good. ⁓ They do the tests. They suggest that what they can offer you is bypass surgery.
your, and you’ve got a weekend, think about it and you, and you go home, do they go, do you go home with medication and joining the medications to keep the blood flowing with anything? What do they do?
Jack Clifford (15:51)
Mm-hmm. Where’d you go? Yeah, such a blessing.
No, no, because I
was leaving against medical advice so they weren’t going to help me, right? And I actually said to the doc, said, you hey, I’m new here because I just moved a couple of months ago to Florida. And I said, can I come see you? And I didn’t have a cardiologist. I didn’t need one before this. And he says, if you live that long, just walks out. So I was on my own at that point. There was no resources of institutional medicine. I had to go find resources myself.
Exploring Alternative Treatments
Bill Gasiamis (16:28)
Wow. Things are pretty wild in Florida. If you live that long and he walked out.
Jack Clifford (16:30)
Yeah.
Yep. That’s exactly what we said. It’s a very sobering moment for me. Yeah.
Bill Gasiamis (16:35)
And you walked out. Yeah, and you walked out.
Far out, man. So what’s the thinking behind walking out of that? Because I understand ⁓ that there are very few things that, like my situation was different, right? But I’ll give you kind of my thinking behind the, I’m gonna walk out routine. It’s like, there is a part of me that sort of says, I don’t need to subscribe to all that medical stuff, all the nonsense. I wanna try and avoid the medications. I wanna do all of that.
Jack Clifford (16:41)
Yeah.
Yeah.
Bill Gasiamis (17:07)
That means I’ve got to do some work to get to that point, right? I’ve got to make sure that I’m eating well. I’m sleeping well. ⁓ I’m exercising. ⁓ I’m not overweight. I’m not smoking. I’m not drinking. Like there’s a responsibility that goes with, don’t want to take that medication. Right. And one of the other things is that, ⁓ if it wasn’t for the medical industry, I would not be here recording this, ⁓ podcast. Yeah. So there’s this big thing, which is.
Jack Clifford (17:31)
Yeah. Double-head sword, right? Yeah. Yeah.
Bill Gasiamis (17:37)
They’re not fixed. My brain is not getting fixed unless they go in and take out the faulty blood vessel and potentially risk all the complications that, that I got the ones I got, but also the ones I didn’t get, which many people get, which is far worse deficits than what I visible on me. So, ⁓ I’m, you know, I’ve never met anyone in my time who hasn’t
Understanding Enhanced External Counter Pulsation (EECP)
who has been through the medical ⁓ system, who hasn’t benefited from it in a way that’s sort of sustained their life, supported their life, lengthened their life. Like everyone that I’ve interviewed has always gone through the medical system and has saved them, supported them, helped them, right? And you’re going to, the first place to get help you’re going to is a hospital, right? You ring up and you go, I’ve got to go.
Jack Clifford (18:22)
Yeah.
Bill Gasiamis (18:31)
to the hospital because I’m feeling like I’m having heart attack. You get there, they confirm it, and then the place that you go to for help is the place you walk out of. What’s the thinking? Yeah, yeah. You have the angina, the blockages. Yeah, you got all of that.
Jack Clifford (18:41)
Well, I didn’t have a heart attack. That’s a really important nuance point. you know, I’m sitting in the hospital all weekend.
there was nothing at risk in an emergent moment for me. My heart wasn’t, you know, I wasn’t going to lose heart muscle if they didn’t do something. Like my mother’s instance was different. She had a heart attack. She probably needed the bypass surgery. It was really hard on her, obviously, like we talked about, but in my case, I had time, but they didn’t treat it like I had time, right?
Bill Gasiamis (18:54)
Okay.
Okay.
Jack Clifford (19:10)
They treated
it like, we’re gonna go in and take care of this thing for you rather than you have time to explore other options when I knew in fact I did. So it might be that getting bypass surgery is the right move for some folks, but it also might be the right move for you and me. We’ve already discussed that you take care of yourself so you never get in that situation. And yeah.
Bill Gasiamis (19:32)
Yeah.
And this is not a interview about do as I say, this is not that interview, right? What this interview is like one person’s experience and what they did. That’s it. We’re not giving medical advice here. We’re not telling you what decisions to make. We’re not telling you any of that stuff. This has got nothing to do with advising anyone to do anything, but what it has got to do with is what either you discovered
Jack Clifford (19:45)
Yeah. Right.
Bill Gasiamis (19:58)
or you knew before and put into action or what you discovered after you left the hospital that weekend. So take us through the next sort of phase of I’m taking responsibility for this and I’m going to take advantage of something that is documented scientifically and proven.
Jack Clifford (20:03)
Yeah. Okay. Yeah. Mm hmm. Yeah.
Yep.
Yeah. And you know, like, so I’ll go into that phase, but, but I just want to share this thing because, know, you, you pretty much already told me when you first heard EECP, you like EECP what? Right. And most doctors are EECP what? Basically every patient is EECP what? And it’s, it’s just, it’s really not going to lie. really bothers me because this, this, this therapy is, is so well-documented. It’s, it’s, it’s FDA approved. It’s not controversial.
Bill Gasiamis (20:25)
Mm-hmm.
Jack Clifford (20:43)
⁓ it just anyways, okay. So, so, so yeah, so I leave the hospital and the only reason I knew about a EECP was because when my mom had her heart attack, I listened to a podcast by Ben Greenfield. He’s a pretty, you know, pretty high-level guy, right? And that had been, that was like 2015. And I just heard mention of it. was like, it was maybe like two minutes of the, of a 60-minute podcast at most, but I was like noted. So I looked into it from my mom. The closest provider was two hours away and you got to go 35 times and my mom isn’t going to drive.
35 times, you four hours round trip. It wasn’t gonna happen, so we moved on, but I just sort of knew about it. And when I say knew about it, I didn’t know, Bill, like what it actually did or how it worked. I didn’t look into it at that level. just, you know, like assessed the situation. I was like, okay, there’s something out there. That’s it. Okay, yeah. It stands for enhanced external counter pulsation. And you want me to go into a little bit about how it works? Yeah, okay, so.
Bill Gasiamis (21:27)
Hmm. And what is a ⁓ CP stamp? What does it stand for?
Yeah, yeah, let’s do that, yeah.
Jack Clifford (21:42)
So EECP involves lying on a bed. From the patient experience, you’re lying on a bed. You have ⁓ cuffs wrapped around your calves, your thighs, and your hips. And inside those cuffs, there are little air bladders.
Bill Gasiamis (21:55)
those cuffs,
are they like blood pressure cuffs?
The Mechanism of EECP
Jack Clifford (21:58)
Yeah, like big giant Velcro blood pressure cuffs. Yes.
Bill Gasiamis (22:02)
Okay, so like they’re much bigger than a regular cuff, which is just over the bicep. Okay. All right.
Jack Clifford (22:04)
Yes.
Yes. Correct. yeah,
just that’s the right way to think about it. you you cinch them up, you’re getting really snug in this thing, but it looks like a giant pantsuit, you know? ⁓ And you lie on the bed and then you get a three lead EKG on you. It’s here, here, in here. And then in between heartbeats, the machine…
inflates compressed air into those bladders at 1.3 psi to start with, which feels like kind of a gentle massage. And then the pressure can be increased in increments of 0.1 psi all the way up to six, which feels like the exact opposite of a gentle massage. However, if you go slowly, your body accommodates to that pressure and that pressure feels different, both over one session and over multiple sessions, meaning
you might not get to six your first session, that’s unlikely, but as you do repeated sessions, you’ll increasingly get closer to six earlier in the treatment and be cumulatively more hours at those higher pressures. And what’s happening is all the blood, not all the blood, a significant amount of blood from your lower body is being pushed up in between heartbeats and it’s causing this phenomenon called sheer stress in your vascular systemically.
And wherever there’s pressure differentials in the body, it’s giving a stimulus to grow. It’s saying the pipes are not big enough, you gotta grow. We’re trying to put through more than is gonna fit. The body’s like, wait a second, it’s not big enough. But growing things in the body takes time. And so you need those repeated sessions. Like I mentioned, T.R., before we started recording, it works just like cardiovascular exercise, but at levels humans can’t do on their own. ⁓ And so, yeah.
Bill Gasiamis (23:52)
That’s important to talk about. so
just for a moment, we’ll talk about that. Like it works like cardiovascular exercise. So the idea with cardiovascular exercise is that what, does cardiovascular exercise do that’s similar to EECP?
Jack Clifford (24:04)
Sure.
If you’re out running, when you hit that stride on your feet, you’re doing that same thing, right? You’re ⁓ sending blood up, right? And then your circulation, your heart’s beating twice as fast maybe than it normally is, or substantially more than you’re just sitting here heartbeat is. And that’s because the heart is responding to the environment around it and saying, I gotta get…
a lot more blood, a lot more places. So I gotta work a lot harder. you know, is maintenance. So collateral blood flow. have alternate routes that we can use that lie dormant throughout our body. And those collaterals, if they never get used, they honestly, they get weaker and they close off, but they also can be reopened, you know? And then you can grow more of them. And…
Bill Gasiamis (24:38)
And what’s the result of that?
Uh-huh.
Okay, so there’s blood vessels that get
less ⁓ blood flow because people are sedentary or people aren’t doing the type of exercise that would activate those blood vessels, for example. And then what in theory, not in theory, and then what happens in cardiovascular exercise, the body goes, we need more blood flow, let’s open up.
Jack Clifford (25:12)
Exactly.
Bill Gasiamis (25:26)
other areas where normally blood flow wouldn’t be required or doesn’t go. And EECP kind of mimics that mechanism.
Jack Clifford (25:27)
Yeah.
Exactly. Yeah, but not kind
of, it’s really important just to note, cause I don’t want, I don’t want any of your listeners thinking, well I’m just going to go run more. Right? I mean, by all means do that safely. You know, the dose always makes the poison with everything, but, but don’t think that you can, you can just go do this. You can do it to a limited degree with exercise, but you’re not going to grow, you know.
that I didn’t have that before. And I like it because it shows you like the world of the possibly or it might be a little unsightly, but it’s feeding my brain. EECP has changed my cognition in addition to my heart, you know, my pelvis and my kidneys and my liver. you know, like it’s, it’s optimized blood flow systemically. Um, yeah. Yeah.
Bill Gasiamis (26:19)
Okay, so let’s go back to the cuff, the cuff
that we put on and then what happens.
Jack Clifford (26:24)
Yeah.
Yeah. So, so you just lie on the machine. Typically you do 35 hours on a machine for a course of treatment and one hour a day is a typical, you know, five days a week. That’s just typically you’re going to the doctor. There’s lots of other variations of that, but that’s the typical course. And that’s the most well-researched course. And, ⁓ you know, over time, usually about halfway through those 35 sessions, if you had angina, you’re going to notice a difference, but
Personal Transformation Through EECP
you know, they use this to treat dementia. It’s a well studied in dementia. There’s a recent study in the US that was profound, a year-long study, a hundred demented patients, roughly a hundred non-demented or a hundred treated patients. Everybody had dementia and a hundred CHAM patients, placebo. The demented patients that got an EECP, they all got better when we know dementia, people get worse in a year, right? They all got better, all of them. And yeah, so that’s like, you know,
similar phenomenon erectile dysfunction, similar phenomenon kidney disease, similar phenomenon stroke recovery. So, you know, these are studies. I’m not making it up. It’s just literally like really well documented. It’s not.
Bill Gasiamis (27:33)
studies
that we can get a hold of and put in the show notes, link to the show notes.
Jack Clifford (27:36)
Yeah, go
to to EECPLocator.com and all these studies are there. ⁓ Yeah. So what I did is in the U.S., I, you know, it’s really hard to find. so I couldn’t find it. I had to, I had to call around and like, I could find a few doctors, none of them near me, but a few of them that would had machines, but they would only use them after everyone had failed stints and failed bypass and they had nothing else to offer them, which makes no sense. But that’s how the insurance reimbursements work.
Bill Gasiamis (27:41)
Okay.
Jack Clifford (28:04)
That’s the only time they’ll actually pay for it. So that’s what they say it’s good for, but that’s not what it’s good for. That’s just what they can get money for, I guess. but, so I had to drive three hours and take a chance on a doctor and stay in a hotel to get my treatments. And it was really difficult. I mean, I ended up buying one of these machines and got it at my house and I’ve just been using it for the last five years. So, you know, 35 hours was great, but I was pretty bad off. Now I got about 700 hours and, uh, you know,
more hours is just greater stimulus to the body to grow vasculature, right? And I mean, I…
Bill Gasiamis (28:38)
how do you know that you’ve grown? I know there’s this ⁓ feeling or this change that happens in the person. ⁓ Like you said, dementia, ⁓ people who experienced dementia have a better outcome later or a change in the way that they’re brain working, et cetera. can you see the, is there a way to see the difference between the blood vessels and
Jack Clifford (29:02)
You can’t, you can’t image, could image
on a, on a cardiac pet would be like the only imaging or I guess, you know, if I went back and did a stress test again, you would, you would be able to see, cause it’s not quantifying specific arteries. It’s, quantifying the total volume, but I tried that they were, actually wouldn’t let me, they said it’s not safe because you have it at a stent or a bypass. So I went back to the same place that I got it, you know, and I was like, literally they put me through the imaging machine. gave me the dye and then they got
Lifestyle Changes and Holistic Health
I went to go on the stress test and the same doctor was there and he refused to tell me to go. So I like, wanted to say, hey doc, let’s go for a run. Cause like, you’re not going to keep up with me, but you know, so I, I didn’t bother with that, but I’ve got my own, you know, I did my own little stress, stress test with a treadmill, right? I started, I was getting chest pain. I found out where I can induce angina and I try and say just below it, you know, so I know where it is, right? I was 2.2 miles an hour. That’s not a fast walk.
And then after the first 19 sessions where I was staying in the hotel, I got up to 2.7. That’s a really big difference even if it doesn’t sound like a lot. And then I got my machine and I kept going. And then within a couple of months, I was starting to do a running stride. And I could keep that up, no angina. I know where angina would come in. I had time calculations and everything. And then eventually, now I can run.
comfortably 6.5 mile an hour pace for quite a while, know, push it up to 14 miles an hour for 30 second sprints and you know, like all kinds of stuff. So, ⁓
Bill Gasiamis (30:38)
How long before
you break the two hour barrier for the marathon? Like was recently done. Maybe, maybe the more blood vessels, the more blood flow. Maybe you can get there.
Jack Clifford (30:42)
⁓ I got zero interest in that. Yeah.
I think so
though, I think those Kenyans should be ⁓ hopping on these EECP machines and they’re I mean, they’re already amazing but.
Bill Gasiamis (30:58)
Well, you want the Kenyans to just completely own marathon running for the rest of eternity. It’s unbelievable what they did. Right. Like I imagine that there is something else going on there, but I imagine blood flow, oxygenation, more blood vessels. Like it’s got to potentially be a thing. reckon if you do a check between the last guy, me, who’s going to like 50 hours before you get to the other side and those dudes, there would
Jack Clifford (31:03)
Yeah, yeah, it’ll just be a Kenyan
Yeah. ⁓
Bill Gasiamis (31:27)
definitely be a difference because they’re exercising all the time, right?
Jack Clifford (31:31)
Sure, yeah, they’re pushing the collaterals as wide open as, know, whatever, whatever a human can do on their own, they’re doing it to the max to, know, the same phenomenon that EECP is doing for folks lying down. You know, they’re doing it to whatever the max you can without the machine, I would say.
Bill Gasiamis (31:48)
So this is a bog standard human body task. Like it just does that all the time. I have heard the blood vessels can reroute in the brain when somebody experiences a blockage and then, and it’s not useful at the time of the blockage, obviously, and it causes potential cell death when somebody has a stroke. But then later on.
Jack Clifford (32:11)
If there’s too much blood,
the revascularization, yeah.
Bill Gasiamis (32:14)
Yeah, so
EECP can kind of occur naturally and then it can support as much of the surrounding tissue as possible so that it doesn’t all die off. ⁓ So what you’re talking about is just encouraging EECP ⁓ to happen more than it would normally happen by ⁓ inducing it through this device where people ⁓ get sort of strapped in and then
Jack Clifford (32:23)
Yeah.
Bill Gasiamis (32:43)
the machine runs, what does it run like a program? Explain how that works.
Jack Clifford (32:47)
Literally,
it’s just air pressure. got different pumps to pump the calves, the thighs and the hips up. And then it’s really just about the timing, right? It’s got to hit it at the right interval of your heartbeat. So it’s at the right place in diastole where your heart is at rest. that timing is very, crucial. And that’s really…
Yeah, it’s not, it’s very old technology. The machine I have was built in 2009. You know, they have new machines that are portable now that I’m working with some of the manufacturers to actually, you know, make these available in the U S because there aren’t any in the U S but they do have portable machines that don’t require a bed. You could get treated on your couch. You could get treated, you know, on your own bed, uh, lying on the floor, I suppose. Um, so, you know, we’ve, we’ve really like technology hasn’t
Bill Gasiamis (33:19)
Wow.
Jack Clifford (33:42)
slowed down. just China’s like taking this thing and you know, have a basically every Chinese hospital has several of these machines and they treat patients in the, in the room with us. It’s, part of their standard of care for all kinds of different, different diseases that they’re treating. You know, and it’s adjunctive to just about everything. There’s nothing that you couldn’t do EECP with, right? ⁓ yeah.
Bill Gasiamis (34:03)
Okay, okay, so.
How do you experience your body differently now? And actually, let’s go back actually, how long has it been since you came across this, decided to get the first treatment, implemented yourself ⁓ at home and then how do you feel different now?
Jack Clifford (34:08)
Oof.
Yeah, it’s been five years
and four months now. And every since like, this is this is a little hard part to quantify, because there’s been a lot of brain changes to from this, right? So so I don’t even like feel like my 47 year old self who was in the hospital, that feels really like somebody else to me. You know, it’s a version of me, I suppose, but I can’t really relate to that person. Because I like a small example.
The Impact of Stress on Health
I used to sleep eight to nine hours a night. That was my normal, my whole life. I was generally like the guy that would come in the latest. You could come to work. was the guy that came in the latest. You And now I get up at two 30 most mornings and I’m like, like rare to go with energy. I’m, you know, I’m working out doing resistance training. I’m reading, you know, I wrote a book, I’m writing another book. I’m writing a book on rectal dysfunction as it relates to this phenomenon, because that’s a whole other, you know, case study.
and I work a full-time job and I just have an incredible amount of energy basically all the time. My mood is way better. My sense of touch is really different now. I give a lot more hugs because it feels really good. ⁓ My sense of smell and taste and…
You know, hearing, you know, I used to like have to go to the bathroom at night sometimes, you know, wake me up to go to the bathroom. Long gone.
Bill Gasiamis (35:47)
So at the same time though, it sounds like also you might have changed other things as well though, right? So what else have you changed in the meantime?
Jack Clifford (35:55)
sure. Yeah. Yeah.
Yeah. It hasn’t just been EECP. Absolutely. you know, really good supplement routine. ⁓ Pretty extensive, but, you know, managing my lipids, for example, I take a thousand milligrams of niacin twice a day. I’ve been able to bring my triglyceride to HDL ratio to kind of an optimal one-to-one, using fish oil and some other things. ⁓ And, you know, I…
I really stay away from carbs for the most part. I like to eat keto, but I like it to be what I call clean keto. So I’m not like pounding keto ice cream or all these things that are, you know, they taste good and yeah, they’re keto, but they got all kinds of oils in them that aren’t really good for your body. ⁓ And, ⁓ you know, I’m big into moving and being active and, you know,
having an engaged social life as much as possible as well. I mean, I think that’s a very underrated thing. That’s actually an area I struggle in because I’m working so much, but you even this helps just, you know, getting to know people even online. But, ⁓
Bill Gasiamis (37:04)
It sounds like you haven’t re it doesn’t sound like you’ve reinvented the wheel. Like everything that you say is things that people take for granted that if they implemented would improve their life before EECP. We’re talking about EECP today, right? But just those things alone would make a massive difference to somebody’s experience. And that’s kind of the message that I’m trying to kind of get into the
Jack Clifford (37:17)
Totally agree.
I thought it a good
Sure.
Bill Gasiamis (37:30)
⁓ minds and hearts of the stroke survivors who I interview and who listened to the podcast. My book, I’m going to, we’re going to talk about your book in a sec, but I’m going to talk about my book. My book, when I wrote it, I thought I discovered all these things that people, should know about that no one knows about, but it’s not true in here is mindset. ⁓ there’s a chapter about emotional intelligence. There’s a chapter about nutrition. There’s a chapter about sleep. There’s a chapter about community.
Jack Clifford (37:32)
Yeah.
Yeah. No, please.
Bill Gasiamis (38:00)
⁓ that’s just the five that I can just rattle off the top of my head right now. And you’ve already mentioned that in the last few minutes, that’s exactly the things that you mentioned. And people take it for granted how much that improves your overall health. Right.
The Journey of Writing a Book
Jack Clifford (38:13)
That’s so true. And also
what’s wrapped up in the wrapper of all of those things that are threaded together is stress, right? ⁓ If you do all of those things, right, you’re lowering stress. How did I get heart disease at 47 when it happened to my grandfather in his late 60s and my mom in her mid 60s and it happened to me at 47? And we know it didn’t happen at 47. It was years earlier and I realized it at 47. Stress, you know? Like I was the guy that took on a lot.
Bill Gasiamis (38:38)
Hiding earlier.
Jack Clifford (38:44)
and had some traumatic things happen in my life and whatever, and I don’t need to go into that. But I always felt like it was all rolling off my back. Like, you know, I’m fine. know, like I didn’t, and there are reasons why I felt that way. ⁓ However, at the end of the day, I know that I wasn’t processing. There was so much I did not process. And I didn’t learn how to like have really good boundaries and that, you know, begot more stress because of those lack of boundaries and, but stress, right? You know, like, but if you have good
good social life and healthy people in your lives, that takes stress off. Eating the right food takes oxidative stress off your body. You could go on and on, but I think stress is gonna kill you before anything else.
Bill Gasiamis (39:17)
you
Yeah. I love
that you said that. I love what I love that. That was the answer that you gave when I said, what else did you do? Because it’s not just, you know, it’s like, I’m going to eat well, but smoke, you know, I’m going to eat well, but drink excessive amounts of alcohol. Like, no, it doesn’t work. You know, you can’t do that. Yeah. can’t do. Yeah. Small.
Jack Clifford (39:42)
No, you gotta do it all in concert. It’s the layers, right? Yeah.
Bill Gasiamis (39:49)
numbers, know, the percentages they add up, you know, 1 % here, 1 % there all adds up and you get a result at the end of it. Okay. So, so you’re you’ve gone, I’m going to see if I can grow new blood vessels to support my heart. And what you’re found between the time that you went to hospital around five years ago to now is that the angina has
Jack Clifford (39:55)
Yeah.
Mm-hmm.
Bill Gasiamis (40:17)
⁓ improved, they’ve gone away. The heart has improved, I beg your pardon, the blood flow. And have you had a medical examination since then to do other comparison?
Jack Clifford (40:28)
Yeah, I have.
Yeah, I’ve got a cardiologist. I haven’t seen him and I’ve talked to him the other day because I talked about the book, but I haven’t gone to see him because he’s a plane flight away. But I’ve been worked up for the crowded intermediate thickness. You might be familiar with that as it relates to stroke. okay, well, they just measure your crowded arteries and look at the placking in your crowded arteries as a proxy for your systemic plaque burden. And flow mediated deletation, is they totally occlude the…
the arm with a blood pressure cuff and then see how quickly you can refill it after, you know, like, it’s like five minutes of this, your hand is completely numb. And those all, you know, workups were good and that was after a couple of years of treatment. You know, I tried to have that stress test, like I mentioned, but you know, now I just see my primary care, you know, he’s a good guy and he runs on my lipid panels and, ⁓ you know, so I’m definitely monitored, but.
What I haven’t done is gotten re-imaged because I don’t want to put extra dye in my system. Sure, somebody wants the images because they don’t believe me, but I’m not trying to sell anybody anything here. I’m just trying to spread the word on something. If somebody doubts my honesty, they can, it’s fine.
Bill Gasiamis (41:38)
I know what you mean, Jack. I know what you mean. I and I asked you because yeah, I would love to see that before and after. would love to see the blood flow. What’s happening, watch change. would be amazing. story to tell, but I also went out of my way if I could to avoid having more dyes and all that kind of stuff injected into my body. I totally get it. It’s okay. Yeah. ⁓
Jack Clifford (41:49)
Yeah.
Yeah. Yeah.
Bill Gasiamis (42:01)
Okay. So you wrote a book about it. Like, what was the idea behind the book? What were you thinking? Show us the one that you got there with the old book cover. And then I’ll include the new book cover in this image as we chat.
Jack Clifford (42:06)
yeah. Yeah. Yeah.
Yeah.
Thanks. Yeah. So I started writing this book, in, know, ⁓ November timeframe, ⁓ after I mentioned to you, so my, my friend came down, ⁓ and stayed with me for 13 days and he had had some stroke damage five years before that was, you know, his whole right side, he just had like numbness and then pain. And then, you know, it this weird cascade of symptoms so bad, you know, sometimes he couldn’t sleep from it. And so
All the time he took off work he could he came and he used the machine three times a day and then he left pain free and like nothing else had worked and then this worked and I didn’t per se expect that I but I was like, you I know it does stuff. It’s helpful. But anyways, when I saw that, you know, I really started digging even more because before that I was like, well, Jesus is amazing. But maybe it’s just me, you know, and and anyways, so, ⁓ so then I, you know, I just started writing the book one day and
The Role of EECP in Heart Health
You know, my mom was a book author and I always wanted to write a book. didn’t really have anything particular to write about and all of sudden I do. So I’m like, you know, let’s see what happens. And, uh, and you dig into the research more and more, and you’re just like, increasingly frustrated by how everyone has known about this. And yet, you know, they don’t promote it. They don’t talk about it because it’s inconvenient. You know, and I’m going to get a little, try not to get like soapboxy here, but
Bill Gasiamis (43:36)
Do
it, do it, go for it man.
Jack Clifford (43:37)
Okay,
okay, because, you know, cardiologists will say it, some of them, the ones that are honest, they’ll be like, like mine. He says, I was making obscene amounts of money, giving people bypass surgeries instance. And then I was given the same people bypass surgeries instance, a couple years later. And, you know, and then he stumbled upon some answers and EECP is one of them that helps his patients stay well. And, you know, he makes a lot less money.
because of it, because he doesn’t go in and do these interventional approaches. And, you know, EECP, the most you could pay somebody is like $100 an hour, and you’re going to tie up a patient room for 35 hours with a tech, it doesn’t make any sense. I go pop a stint and you make 10 grand in two hours and never see you again. You know, like it just, I get it from, you know, I want to own a portion of Ferrari and have a lake house and a winter house, but
You know, like, I don’t know how you live with yourself. You said go for it, man. I’m going to go for it. you know, and my son’s about to graduate. Okay. Yeah. Okay. Fair enough. I’m good with it. Yeah. Yeah.
Bill Gasiamis (44:38)
But come on, come on, Jack. Yeah, you go for it. I’m going to push back. I’m going to push back as well. You go for it. I’ll push back. There’s yeah. Which is cool. Right? That’s what I want. I want to have a conversation and
I don’t want to control the narrative, but the guy that goes in needs a stint today has a blockage. Like that’s life saving. That does work. What I am afraid of that happens sometimes when people go in and they’ve got a blockage and then they get ⁓ even even a stroke blockage. Right.
in carotid or a vertebral artery. What happens is sometimes people go in and they get told you need a stent. Fair enough. You’re about to have a heart attack. You’re about to have a major stroke. If we don’t put one in, you’ll have a, that’s necessary. The challenge is, that that person sometimes doesn’t learn the lesson of what got them into the situation where they need a stent.
Jack Clifford (45:22)
Good.
Exactly. sure.
Yeah, by all means. Like emergency medicine is great. And we’ll put that in the emergency medicine category of cardiology, right? Why aren’t they offering you, why aren’t they saying, Hey, you’re at risk for a whole lot of other things just by this happening. Why don’t you come 35 times to this EECP machine and you know, like, or why don’t we have centers
Bill Gasiamis (45:36)
Yeah.
Yes, and then later…
Jack Clifford (45:55)
all over. I found exactly one place in Australia so far that I’m not focusing on Australia right now. I do plan to take EECP Locator International, but right now the access points in the US are abysmal. 70, 80 % of the people in the United States could not get to a center. There’s no access point that’s at all realistic for them to get to. And yet these machines are not that expensive. They’re the price of a
Decent not that great car. ⁓
Bill Gasiamis (46:24)
we’re starting to
see them in, I don’t know, health spas or something like that, where people will go, they’ll get yoga, they’ll get this, they’ll get that, they’ll get infusions perhaps and all sorts of other things. And there’ll be a machine or there’ll be a suit that people can put on and they can go through one hour.
Jack Clifford (46:29)
Yeah, that’s good.
That’s great.
Yeah, although
I do want to say that the Normatech, like the compression boots that they have and some of those things, when they don’t use the pressures that EECP uses up to 6 PSI and they’re not sinking it in between heartbeats, it’s helpful, but we’re not talking about things that can do the same thing in the body. It’s on the right path and I’m not digging it as being worthless because it’s not, but it’s just not the right thing.
Bill Gasiamis (46:47)
Yes. Yeah.
Yeah.
Yeah, that’s kind of what we’re seeing. And to go back to your point is because the medical profession does medical profession stuff. this is not, it’s not that it’s not medically kind of aligned. It definitely is. But when you’re told that the way you solve a problem is through putting a stent in and then never talking to that patient again, to tell them how to avoid to get a stent in that’s
Jack Clifford (47:31)
Yeah, that’s your job.
Bill Gasiamis (47:34)
what they do, like they’ve been trained to do that forever. And that’s what they do. And that works and it saves the life. But what it doesn’t do, which I also have a challenge with this, it doesn’t teach the lesson. What it reinforces is that if I have something wrong with me and I go to a doctor, they’ll fix it. So next time it goes wrong, I’ll just go to the doctor and they’ll fix it again. And I didn’t have to change my life. Like this even bloody advertisements that do that. They
Jack Clifford (47:51)
just I’ll go and he’ll fix it.
Yeah. Yes. Yes.
Bill Gasiamis (48:03)
They hijack that part of the person’s brain and they say, you know, have you got reflux, heartburn, that kind of stuff? Don’t let reflux and heartburn get in the way of eating the foods that you love. Just take a tablet. You know, that’s the same kind of thing, right? And that’s why the medical profession doesn’t do that because they’re not trained to do anything other than sell their thing. And their thing is what they went to work, to school for.
Raising Awareness for EECP Therapy
Jack Clifford (48:17)
Yes.
Bill Gasiamis (48:30)
20 years to be able to administer. But every so often you come across an amazing doctor, surgeon, et cetera, who says, I can’t do anything more for you, but maybe somebody else can. Those guys are better than the doctor who says, we can’t do anything else for you and then send you off their way. That next sentence, but maybe somebody else can, I don’t know who they are. That is.
Jack Clifford (48:43)
Mm-hmm.
Bill Gasiamis (48:57)
I think a great thing to say this is where I think EACP kind of fits in that now that I’m here and things are not good.
Jack Clifford (49:05)
I totally agree. I totally agree. And
yeah. And you, so you, you mentioned like the wellness spas and whatnot. And here’s the thing in 2015. So, you know, somewhat recently the FDA approved EECP for a brand new indication, general circulation, right? In healthy people. Like it’s right on the FDA indication. And also in one case in increase in VO2 max, but rough, that’s roughly saying the same thing. ⁓ yeah.
Bill Gasiamis (49:32)
for healthy people, was that part
of it?
Jack Clifford (49:35)
Yeah, it said unhealthy patients and healthy people didn’t call patients. So, so, ⁓ but, but, know, the litmus test for that is, is your doctor say you’re healthy enough to undergo circulation enhancement? If the answer is yes, you know, it doesn’t matter if you got all that other stuff or not, you know, we’re just not treating you for it. We’re not saying ECPs is fix for this, your erectile dysfunction. It might help it. You know, what’s not saying it’s, it’s the fix for your stroke, but it might really help your stroke, recovery, but.
Bill Gasiamis (49:47)
which
Jack Clifford (50:03)
Anyhow, so like you can, you know, I don’t know about in Australia, but in the United States, you could get an EECP machine and create a viable business model off of helping people as soon as people actually know about it and what it does, right? I’m trying to solve the access issue in the United States by aggregating demand, right, as one of the solutions. So I have a website, eecplocator.com. And if people… ⁓
tell me that they like EECP to be available in their area, when I get like five to 10 patients in one area, we’re gonna find a way to get it to them. ⁓ The how is, you there’s a bunch of different possible ways we can get EECP to them, but at the end of the day, you know, like people need this treatment. They really, really do.
Bill Gasiamis (50:50)
Yeah. We’re
not talking about anything ⁓ out there. Like this is not an out there thing. This is definitely common. Now I, I don’t know how I haven’t come across it. I’ve all these years after all these years now I’ve just because of our conversation right now, I just did a Google search and I typed in EECP machine Australia. And the first thing that came up was an Australian government department of health, disability and aging.
Jack Clifford (50:57)
No, it’s that.
Bill Gasiamis (51:20)
document from the Therapeutic Goods Administration, which
talks about a mid-trade Australia EECP system model, external counter pulsation system stationary. So it seems like they have a…
Jack Clifford (51:36)
Like they’ve approved it, sounds like they have some approved devices. Yeah.
Bill Gasiamis (51:38)
Something like they’re at least looking at it. Let me see what that
says. The inclusion of the kind of device in the AI community is subject to compliance with conditions placed in post. Yeah, it sounds like it’s been through some regulated body in 2021.
Jack Clifford (51:52)
Yeah. Mm-hmm.
Yep. There you go.
Bill Gasiamis (51:57)
This device is intended to provide external counter pulsation therapy and is indicated for use in the treatment of stable angina.
Jack Clifford (52:06)
Mm-hmm.
Bill Gasiamis (52:08)
pectoris and congestive heart failure. There you go, my friend.
Jack Clifford (52:10)
Yeah, it works great for
people with art failure. It really does.
Bill Gasiamis (52:14)
Dude, father-in-law had heart failure. He passed away from heart failure just a few, about a year and a half ago. ⁓ Now, I don’t know, I’m not saying anything, but we’ve never heard of this before. Today’s my first time where I’m really going to deep dive about this thing with you. ⁓ So what are the challenges that you face? what are the, what is it? ⁓ The barriers that you face?
Jack Clifford (52:20)
Yeah.
Bill Gasiamis (52:44)
when you’re speaking to people about this or how people finding out about it, how do you help people like
Jack Clifford (52:50)
It’s just an awareness piece. It’s an EECP what? And then, you you get in with some physicians and then you got to duke it out a little bit. Not with all of them. There’s plenty of physicians, you know, I’ve talked to the physicians that have machines and are doing the right thing for society and still making plenty of money. ⁓ They’ll just tell you, you know, I’ve talked to some cardiologists and just they know that all their colleagues are, you know, kind of crooked in certain ways. But
Bill Gasiamis (53:03)
Mm-hmm.
Jack Clifford (53:17)
⁓ Or at least they just haven’t taken the time, you know, like it’s a matter of what catches your shiny attention, right? Like you’re gonna, I know that’s fair. I want to retract that. I do.
Bill Gasiamis (53:20)
Yeah, let’s not call them crooked. I want to feel
like they are just not aware or they are
Jack Clifford (53:32)
Yeah, no,
and think that’s accurate, but I think maybe a more accurate thing would be to say not curious. It’s the lack of curiosity that bothers me. ⁓ I don’t need to go into it any further than to say like, hey, ⁓ some people know about it. Plenty of people haven’t bothered to find out that probably should have. ⁓ But in either case, we are where we are. ⁓
We’ve got a giant access crisis, but China has 5,000 access points. We have 150. I don’t know how many you have in Australia, but it’s not enough. let’s fix this because this could change the health status of your entire country, of the world. Like if people were proactively getting 35 hours of VECP, it’s some kind of an interval when they’re in an at risk.
category, which we can quantify with various tests and measures, you could easily stop people from ever getting to your father’s situation. My dad who died of dementia situation, sorry, father in law, yeah. ⁓
Bill Gasiamis (54:36)
Yeah, other in-laws. Yeah.
I hear you. hear you. Maybe what we need to do is maybe we need to, ⁓ get some data out and say how bad this is. Like it’s, we’ll call it something as bad as smoking and then we’ll get an advertising company to create a marketing campaign about how something bad is good for you. And then we’ll just teach people to be addicted to doing something good for themselves that they don’t know is good for themselves. Maybe that’s the way in. I know, I know where you’re coming from. get it.
Jack Clifford (54:58)
Yeah, right. There you go. We’ll reverse psychology.
Exactly. Yeah, although I want
to comment on one little side piece of benefit of the machine, which is I didn’t discover this right away and in 35 hours, probably not enough to do it, but you can appreciate the value of breath work, I believe, right Bill? And on the machine, it’s going to dunk, to dunk, to dunk at the rate of your heartbeat. If you learn to…
Bill Gasiamis (55:22)
Yeah, yeah, that’s huge.
Exploring the Future of EECP Therapy
Jack Clifford (55:31)
You slow the machine down like 30 beats a minute. You know, it’s real dramatic. goes from the dunk, the dunk, the dunk, to the dunk, to dunk, to dunk. And it’s just really crazy biofeedback in addition, because the pressure in your hips, right? It’s doing this to you. It’s strengthening your core and you really get to learn how to do breath work on the machine. And what I’ve found is over these 700 hours now, I have reflexive breathing. When I’m stressed out, don’t hyperventilate. I do the opposite.
it’s reflexive. And that’s because of those hours on the machine and just using that time, that time you’re stuck there for an hour. You guys will do some stuff.
Bill Gasiamis (56:14)
Yeah. I imagine it makes you feel really well. Also afterwards, I imagine like you’re meditating or you’re focusing on your breathing. Plus it’s doing that. Like the whole experience one hour or giving yourself one hour of time to do that is an amazing experience anyway.
Jack Clifford (56:18)
It does.
Mm-hmm.
I agree, totally agree.
Bill Gasiamis (56:33)
Yeah. ⁓ so let’s just get back to the book a little bit. Like, how does it go through? What does it go through? it scientifically based? What’s the idea with it?
Jack Clifford (56:41)
Yeah, yeah,
my story and you know a little bit about my wife’s journey along with me because it’s really benefited her as well too, but ⁓ She doesn’t have as many hours as I do and then we talk about ⁓ The you know the differences between other countries like China and India and why and what you know They’re different for both countries and some other countries where it’s more advanced And then we talk about the different, know how it works and what it works for and then we talk about
⁓ how a patient could actually go about, you know, accessing this therapy in the United States. And then we talked about kind of the future of the world of the possible if the EECP access was a thing and you how much money it could save our government and know, healthcare dollars or at least healthcare dollars could be spent better. ⁓ And
That’s about it. But it really helps you understand if you’re in the why haven’t heard of this camp before, you’ll really understand why. It’s very, very particular about picking apart what happened and why it kind of… So it had it like it’s high watermark was probably around 2006. And then drug eluding stents came out and people kind of lost interest in the EZP in the US. And so it just went a different direction.
And then here China with medicine, know, incentives that are different than ours, you know, it expanded from there and we were trying.
Bill Gasiamis (58:10)
Yeah, I love it. ⁓ so I, while you were chatting and I did it, I did another search for a CPM machine image photo. And there’s a Australian organization that has, ⁓ a machine that you lie on that they wrap you up in and it takes you through that process as well. Okay. So I’m just, I can’t believe I’m just becoming aware of this. They call it. They, they, one of their, ⁓ offerings is mitochondrial cell training.
Jack Clifford (58:37)
Yeah, I don’t disagree. I mean, when you deliver it, when you get so much blood flow in these small little capillaries that are the size of a human hair, right? You know, there’s a profound change at the cellular.
Bill Gasiamis (58:40)
Yeah, yep.
What I like about it is ⁓ if there is a therapeutic goods administration kind of approval and these machines are appearing in, we’ll call them ⁓ medical centers or health wellness centers or wherever, ⁓ clearly there’s.
a lot of benefit, very little risk. And then therefore people are feeling comfortable promoting this. This particular organization, I won’t name them, they have medical in ⁓ in their title, which sort of suggests that they are kind of maybe general practitioners or doctors of some sort. There’s a link, I’m in Melbourne, there’s a link that says new to Melbourne and it’s got an organization that’s there as well that talks about it.
Jack Clifford (59:11)
Yes.
Nice.
Bill Gasiamis (59:37)
So there you go. It’s more well known than I could ever have thought. And then there’s a video battling AONOCA angina and dyspnea after the COVID vaccine is one of the videos. yeah, look, doctors names listed all over here. Interviews. Okay.
Jack Clifford (59:41)
Yeah. That’s a start anyway.
Bill Gasiamis (1:00:04)
This is brilliant. I didn’t come in here skeptical, but I had never heard of it. So I didn’t even know how to start this conversation, but I love the idea of being able to offer solutions to stroke survivors who would benefit from additional blood flow, blood vessels, reroute around the damaged areas in their brain. ⁓ It’s kind of what hyperbaric oxygen therapy ⁓ aims to do as well.
Jack Clifford (1:00:23)
So.
Yeah, yeah, they go
hand in hand. The two are probably really powerful together. just, EECP works, but I’ve owned a hyperbaric chamber. I’m actually really familiar with it. ⁓ And I think a lot of it, but it’s really, it’s uncomfortable. And, you know, EECP can be uncomfortable in its own way, but it’s not, it’s not, you know, if you’re claustrophobic or if you have, you know, ear pressure sensitivity, ⁓ you know, hyperbaric has its challenges. ⁓
Bill Gasiamis (1:00:36)
Yeah.
Jack Clifford (1:00:55)
But it’s not going to grow blood vessels. It’s not in the same way. It’s going to oxygenate what you have. The EECP is going to give you a lot more. ⁓ They would work really well together. ⁓ Anyhow, ⁓ the one thing I want your listeners to just keep in mind is, it works just like exercise. So it’s gradual. So you’re going to get into it what you put out of it in terms of hours on the machine. ⁓ There are ways to get machines.
Bill Gasiamis (1:01:02)
I
Jack Clifford (1:01:22)
So if anybody, feel free to reach out to me. If you go to eecpbook.com, I’ve got all my contact information. I’d be happy to have a discussion with anyone. I’ve got a contact to my Facebook group and I’m talking to people from all over the world there. ⁓ I don’t charge anything to consult with people. I just passionate about EECP and spreading the word. yeah, it ⁓ sounds like it’s already approved in Australia. So that’s great. That means they could ship you a device if you wanted to. ⁓
One of the things that’s been really neat, we’ve been working with lot of couples lately and they’ll treat each other on our machine. They’ll stay with us for a couple of weeks and do that or stay near home. In the US, I’m open and I’ve got a space, like a six unit Airbnb. People will come and just stay there and get the treatment done. They’ll get the 35 hours done in 18 days, so it’s a lot faster instead of seven weeks.
Bill Gasiamis (1:02:15)
Mm-hmm.
Jack Clifford (1:02:17)
But the couples thing is actually a really big deal. I will say this, like, I don’t have the picture. I just posted it on my Facebook group, but it shows the different parts of the body and the blood flow increase. And let me just say the pelvis stands out about four act. So I like to say, like couples should really be doing this together. It’s almost a little dangerous for them not to.
Bill Gasiamis (1:02:31)
Uh-huh. Uh-huh.
Yeah, I hear you.
hear you. It could actually probably help some men in, you know, ⁓ erectile dysfunction issues. Like I get that as well. Like it makes complete sense. we’ll diet, so we’ll not smoking, so we’ll not drinking, so we’ll exercising, so we’ll not eating carbs, ⁓ and increasing your testosterone through, you know, physical activity and all that kind of stuff. Like all those things go hand in hand, right? And
Jack Clifford (1:02:55)
Yes, all these can be done.
Bill Gasiamis (1:03:09)
If you can give it a boost as well with this thing, that’ll be, you know, that’s amazing. Again, non-invasive, ⁓ everything about it sounds like it’s good. I’m glad we had this conversation and I’m going to look into it a lot further. Thanks so much for reaching out. We will have all the links in the show notes so that anyone who wants to reach out and ⁓ catch up with Jack. ⁓ I love your story, man. Thank you so much.
Jack Clifford (1:03:33)
Yeah, thanks Bill. This has been fun. Really appreciate it.
Bill Gasiamis (1:03:36)
That was Jack Clifford, and I want to thank Jack for taking the time to walk us through the science and his personal experience with EECP therapy. So what stays with me from this conversation is the biology. The idea that the body already has dormant bypass channels and that under the right mechanical stimulus, it can be told to activate them and that it’s not science fiction, that it’s arteriogenesis.
and it changes how I think about what’s possible in stroke recovery. But I do wanna be clear one more time, EECP therapy is approved in Australia for stable angina and heart failure. I’m not sure what the status is in the United States, but I think it’s similar. It is not approved for stroke. This is emerging off-label research and everything we discussed today is for informational purposes only. So please speak.
to your treating doctor before pursuing any treatment. If you want to explore EACP further, find the provider at eecplocator.com and learn more about the therapy at eecpbook.com. The research we referenced today was a 2026 meta-analysis from the QJM across 15 studies and 506 participants. The link is in the show notes.
If today’s episode sparked something in you, I’d love for you to grab a copy of my book, The Unexpected Way That Stroke Became the Best Thing That It’s the resource I wished I had had in own recovery in the early days. And you can get it at And if you want to support this podcast and the work of getting evidence informed, honest conversations about stroke recovery out into the world.
join us at can sign up there and you can support the podcast for as little as $6 a month. Until next time, keep recovering. I’m Bill Gasiamas. This has been Recovery After Stroke.