Understanding the anatomy of the brain is something that stroke survivors may benefit from when trying to comprehend how a stroke has impacted their body and personality and their health.
Socials:
www.instagram.com/theanatomynerdpodcast/
Highlights:
02:41 Introduction
03:30 Hilary Helt
06:09 What Is Kinesiology
09:01 Anatomy Of The Brain
16:52 Change In Personality
28:48 The Brain Is Changing
32:54 The Parietal Lobe
42:28 The Occipital Lobe
46:42 The Cerebellum
Transcription:
Hilary 0:00
So the parietal lobe is really interesting. I like the parietal lobe because it has to do with touch. So like we have these different neurons that like the very tips of our skin, that senses touch.
Hilary 0:13
And they just have like, these really crazy names and like, there’s all these weird shapes, like one is kind of like a funny little oval, and it just like gets smaller and smaller and smaller.
Hilary 0:23
Like there’s different neurons that sense, pressure. And there’s different neurons that sense pain. And that all goes to your parietal lobe when you’re sensing all of that. And then there’s others that sense temperature.
Hilary 0:37
So like if you’re going to, you know, touch that hot stove, right? That’s always the example why does everyone always use that example?
Bill 0:43
Because it’s so true.
Hilary 0:47
Yeah, and then your neurons are gone to that parietal lobe. Don’t touch that. That’s hot.
Intro 0:55
This is the recovery after stroke podcast, with Bill Gasiamis, helping you navigate recovery after stroke.
Bill 1:08
Hello, and welcome to recovery after stroke, a podcast full of answers, advice and practical tools for stroke survivors. To help you take back your life after a stroke and build a stronger future.
Bill 1:19
I’m your host three times a stroke survivor Bill Gasiamis. After my iron life was turned upside down, and I went from being an active father to being stuck in hospital, I knew if I wanted to get back to the life I love before, my recovery was up to me.
Bill 1:35
After years of researching, discovering and learning how to heal my brain and rebuild a healthier and happier life than I ever dreamed possible. I’ve made it my mission to empower other stroke survivors like you to recover faster, achieve your goals and take back the freedom you deserve.
Bill 1:54
If you enjoy this episode on what more resources, accessible training, and hands-on support, check out the recovery after stroke membership community created for stroke survivors and caregivers.
Bill 2:05
This is your clear pathway to transform your symptoms, reduce your anxiety and navigate your journey to recovery with confidence, head to recoveryafterstroke.com to find out more after this episode, but for now, let’s dive right in.
Bill 2:21
This is Episode 151, and my guest today is Hilary Helt the host of the anatomy nerd podcast and in today’s episode, we discussed the different lobes of the brain and how a stroke in one of them may impact your body and your personality.
Introduction

Bill 2:41
Hilary Helt Welcome to the podcast.
Hilary 2:44
Thank you so much, Bill. It’s so exciting to be here, thank you for having me.
Bill 2:49
Exciting to have you here. Now that I know that you’re very proficient in cleaning up spills and solving problems and fixing things. Did you need to go and get some more kombucha?
Hilary 3:03
I’m okay. I’ve got a sip left. But you know, yeah, right before we press the record button kombucha everywhere. I’m used to cleaning up spills, I’ve got a toddler. So just another one to clean up.
Bill 3:19
Your you’re the founder of the anatomy nerd podcast. But before we talk about that, tell me a little bit about you and what you do.
Hilary Helt

Hilary 3:30
So I am a podcaster and a mom, those are my two big roles for right now. But my past is a little bit more telling of how I came to be a podcaster I fell in love with the human body and how it works several, several, several years ago in undergrad.
Hilary 3:50
And I decided to get my degree in kinesiology. And kinesiology is the study of human body movement. And that was getting me on the path to become a physical therapist. So I studied that for several years and was getting into PT school and all that jazz.
Hilary 4:08
And in the interim, I was in PT clinics and hospitals and all that jazz and just working with patients with several different things going on needing rehab. One of them being strokes.
Hilary 4:25
And then you know, a really common one is like knee replacements and shoulder surgeries and all that stuff. But you know, my love for the human body had kind of started then and has never really gone away.
Hilary 4:41
A little bit of what happened with PT school as I got in, but I decided not to go. And so that led me to other avenues in my life. One of them being this podcast. So I am the host of the anatomy nerd podcast and I really just love that it’s just an educational piece for anyone.
Hilary 5:02
You don’t have to have a degree in kinesiology or, you know human anatomy or you know biology or what have you to tune in and learn a little bit and nerd out a lot a bit about the human body. So that’s what I do.
Bill 5:21
In a little bit we’re gonna nerd out on the brain. But first, we got to talk kinesiology. Because what is that? It seems really weird and bizarre. I’ve been the recipient of Kinesiology sessions, I suppose.
Bill 5:34
And it’s so weird and bizarre, I do not understand it at all. But I really enjoy it, I enjoyed, and I appreciate it. And what’s really weird is that, you know, there’s a guy or a girl depending on who you go and visit who you know, they touch something at some part of your body and it changes something at another part of your body, proving the concept of you know, the hip bones connected to the thigh bone, the head bones connected to that bone, and all that kind of stuff.
Hilary 6:05
It’s all connected in like a really funny way.
What Is Kinesiology – Hilary Helt

Bill 6:09
Tell me about that. Tell me about Kinesiology and what it is if we can give people an understanding of what it is and then how it helps, because I’ve definitely benefited from it. Since the stroke and even before the stroke.
Hilary 6:22
Yeah, so at its very basics, kinesiology is just the study of human body movements. So we’re talking about, like, what goes on, in your body, when you take your arm from slack to moving it up, and you have a cup in your hand, and maybe you’re knocking over a cup on the table.
Hilary 6:40
It’s studying, like the force that your your bicep and your tricep are using to lift that arm up, and that the nerves that are coming through down your brain to your spinal cord out into the muscles to fire those muscles to make those muscles move and all that jazz.
Hilary 6:56
So it’s a study of how your body is working to make all of that stuff happen. And you can get really, really deep into like the biomechanics side, like studying exactly like the amount of force, it’s going into the muscles to lift that glass.
Hilary 7:13
Or you can go you know, into the major, like biochemistry part of it, like studying the actual you know, chemicals and hormones and all the little nitty gritty bits like that, that go into, you know, making that muscle move and like making, you know, your calcium channels open and all that stuff.
Hilary 7:34
Like it gets really complicated in that avenue. So the specialty that I went into for kinesiology was Exercise Science, because, you know, like I said, I was going to be a physical therapist.
Hilary 7:48
And so with all of that study that is mostly just kind of just focusing on how the body moves, and how the body doesn’t move when something is wrong. So that kind of ties into our theme for today’s episode talking about strokes, right? Because when you have a stroke, that’s when kind of things go a little bit off.
Bill 8:13
A lot of people seem to get the impression, and it’s the way they talk about it is that my hand doesn’t work or my leg doesn’t work, but it’s actually not the hand or the leg that’s not working.
Bill 8:24
It’s the brain that’s impacted, that’s causing that connection to be different. And therefore the feedback isn’t going to the brain, it’s not that the hand and leg don’t work, it’s that the information is not getting back to the brain, so the brain doesn’t know what to do with that arm or leg, is that accurate?
Hilary 8:43
That’s 100% accurate. Yeah, so when you have a stroke, you know, it’s often a brain bleed, or a brain like a blood blockage and so that means that like the brain isn’t going to work as it should, it’s not going to be able to send those messages.
Anatomy Of The Brain
Hilary 9:01
So you have your brain and your nervous system is kind of divided into two parts, you’ve got your central nervous system, which is your brain and your spinal cord. And then you have your peripheral nervous system. And that’s like all of the nerves that come out of your spinal cord and like down your limbs and down to your to even to like that very down to the very tip of your toes.
Hilary 9:21
That’s your peripheral nervous system. But it all kind of starts with our big, beautiful brain, you know, and when you have a stroke, depending on where you have the dysfunction in the brain due to the stroke, it’s going to kind of affect how you know what’s going on in your body.
Hilary 9:39
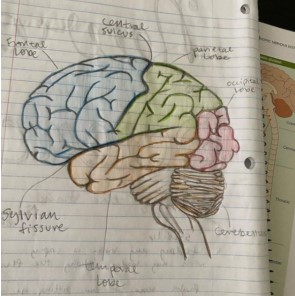
So say you have a stroke in your frontal lobe. So like right here, so let’s kind of, you know, describe the brain a little bit so it has lobes. So the frontal lobe is right here kind of makes sense front.
Hilary 9:54
And then you’ve got your parietal lobes kind of right behind it. So like right kind of here, you can kind of see, and then you’ve got your temporal lobes on the side, kind of right behind your ears, and then your occipital lobe right in the back.
Hilary 10:09
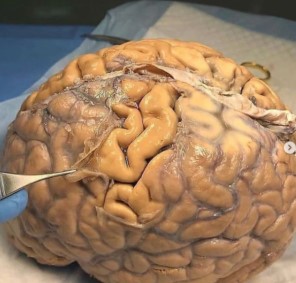
And then, so like the brain is connected into its two sides, and then it’s connected in the middle. And then you have your brainstem and your cerebellum in the back this like little like mini brain, it’s called like that the baby brain in the back, and that’s kind of like tucked right on in there.
Hilary 10:27
It’s like, right at the nape of your neck. And then it goes down to the brainstem into the spinal cord, the spinal cord is like that big, you know, mother lode, that’s like, we’re all of that the direction is happening, that’s like the big four way stop, you know.
Hilary 10:42
That’s where everything is happening where all the direction start going, and then all of your spinal nerves that come off, and then go down, you know, down to your arms and your legs.
Hilary 10:54
So but so the different lobes, the frontal lobes, and the parietal and all that jazz, that’s kind of what we’re talking about when we’re talking about injuries involved in brain injuries involved with strokes.
Hilary 11:07
So for example, if you have a stroke in your frontal lobe, the frontal lobe is mostly involved with like your personality, your behavior, you know, your mood, and stuff like that. So if you have a stroke, right there in the front, those kind of things are going to be really changed and really affected.
Hilary 11:30
And, it’s kind of wild, because it’s really, really different for everyone. one stroke in one person is going to look, even if it’s in the exact same spot, which is very rare. But if it’s in the exact same spot in two different people, it’s going to present differently. So it’s kind of wild.
Bill 11:50
So when the stroke happens in the frontal lobe, is it the frontal lobe on the left of the head, and the frontal lobe on the right of the head do different things, or do they do similar things, but differently?
Hilary 12:04
That’s exactly it, that’s more accurate. I’m glad that you mentioned that, because that’s actually a really important detail that I left out. So we have our left and right lobes. But and they do so like your, you know, the lobes work similarly, but differently, if you have a injury on the left side, your right side is going to be affected.
Hilary 12:26
Because one half the left side of your brain controls the right side of your brain. And the right side of the brain controls the left side of your brain, or the left side of your body, excuse me, I may have said that on but just think of it as it’s switched, which is really kind of funny.
Hilary 12:41
And that happens that the brain stem in the back. And it’s just, it’s just like, No, I don’t recall the explanation of why that is right now. But it’s just just kind of how we’re built. So if you, if you have an injury in your, you know, your right side of your brain, you’re likely going to have you know, something going on, on your left side, just remember that, which is weird. It’s not something that you that’s not how you would imagine it happening, right. But that’s how it is.
Bill 13:08
So that happens at the brainstem?
Hilary 13:14
That switch it’s like a neural pathway. So like, neurons are really interesting, right? It’s like there’s a, there’s a million neurons in the pathway that goes from like, the action in your brain to your fingertips or your toes, or whatever it is, you know, there’s a million neurons that are all connected, that, you know, make that actually happen. And that switch happens between some neurons in your brain stem right back here. It’s interesting.
Bill 13:43
Okay, so that, so then, people who experience a stroke in their frontal lobe, it might impact their personality. So for people that are listening, who are caregivers, or even stroke survivors, what are some of the changes that might happen if somebody has a stroke in the frontal lobe? As in how does their personality change? I know there’s a whole bunch of different you know, there’s probably, limitless ways, but give us a bit of a couple of examples of how that might change.
Hilary 14:23
Yeah, no, that’s a really, really great question. Especially since it you know, as you said, it can be different for everyone. It could be as simple as you know, let’s say Jane had a stroke. And she used to be a really easy going down to earth gal and you know, you would throw something matter and she’s like, okay, cool, let’s go.
Hilary 14:42
And then suddenly, after her stroke, you know, she’s just not, you know, it’s however much time after her recovery, and she’s just kind of not as easy going. She’s kind of, you know, really wanting to stick to a schedule. You know, she’s like a little thrown off if her schedule is thrown off.
Hilary 14:59
You know, she’s just really kind of not as easy going, you know, it could be something like that. Or it could be somebody who was more high energy is just kind of has like a more flat effect, it could be something like that, too. So it really, really is so different for everyone. I don’t think that I can stress that enough.
Hilary 15:21
And I think that, you know, your listeners who have experienced strokes before can definitely, definitely let that you know, that will resonate with them. And you know, that they’ve probably have spoken with others who have had a similar stroke to those and like, well, yeah, I felt this way and this way, and then you feel that way, in that way.
Hilary 15:36
And it’s just, all, it’s all different. You know, that’s, it’s kind of what’s really tricky about the brain. And what kind of fascinates me is that, you would think that it’s all the same, right? Like this part makes you feel that it’s, and this part makes you taste that and this part moves your right leg.
Hilary 15:50
And you know, you would think that, okay, if I have a brain bleed I’ve had burst blood vessel that it would just kind of shut that off, like a light switch, right? But it’s not, it’s tricky.
Bill 16:02
Yeah, and people who experience a change of personality. Often, the family members or the loved ones think that they’re doing it on purpose, or they’re being lazy, or they tend to label that it tends to be a really difficult thing to overcome, because fatigue might be causing a change in personality alone, let alone an exact challenge in the frontal lobe.
Bill 16:29
And then it’s hard for people to express themselves as well as to why they’re behaving a certain way, they might not even have an idea that they’re behaving a certain way, it’s quite complex. In that, I have a lot of caregivers who contact me and say, you know, my dad, my son, brother, whoever is had a stroke.
Change In Personality

Bill 16:52
And now they won’t do this. And they won’t do that. And they’re behaving like this and they’re behaving like that. And I really don’t understand it. And it’s frustrating, and it’s annoying me, and they don’t realize that just as a result of the stroke, that person may not be doing it intentionally.
Hilary 17:07
It can be really hard when your loved one is completely different after a stroke, right? Especially if you’re, I mean, you know, you your loved ones have been the same way that same person for as long as you’ve known them, right? And then suddenly, they’re a different person.
Hilary 17:21
And it’s an it can be really challenging. And the biggest thing for the, you know, stroke survivor, and for the family member, or the caregiver to remember is to just to be patient, you know, every day, even Every moment is different in stroke recovery.
Hilary 17:38
And those differences, they might be temporary, and they may not be and you just kind of have to remember to be really patient with yourself and be really patient with, you know, your family and that, you know, it’s gonna get better. It is, you know, but also just accept that man, it’s friggin hard. It’s just hard, you know, and gave yourself a lot of grace for that.
Bill 18:08
Yeah. Right tips. So what does the temporal lobe do? What’s the point of that?
Hilary 18:14
Yeah, so the temporal lobe is a little bit different. So it is involved in like, understanding memory. And then understanding language. So that can be like, there’s a part called the wernickers area. And if that part is affected, and like your ability to like, you know, convey and and like, understand, communication is affected and is really difficult.
Hilary 18:45
Hearing is also proud of the temporal lobe, depending on where that stroke is. And then sequencing and organization. So like, getting that like, this piece goes here, and then this piece, versus this piece goes here. And then that piece, if that makes any sense.
Hilary 19:01
So like, maybe organizing a phone book would be challenging, or maybe organizing your kitchen or like, Oh, wait, where does this cup go, you know, something as simple as that is like a, you know, a stroke survivor trying to just empty the dishwasher, you know, they’ve grabbed that cup out of the dishwasher, and they’re like, cool, I don’t remember where this goes.
Hilary 19:22
You know, something is hard. And as you know, just challenging is that it can be what happens and it’s just a it’s a funny little area of the brain because it covers a lot like, there’s how a lot of different things like language and memory and hearing like that’s all very different.
Hilary 19:40
And it all can be affected when you have a stroke in that area. Memory is a tough one because, you know, you’re already kind of dealing with like the confusion and the fuzz. After after a stroke.
Intro 19:53
If you’ve had a stroke, and you’re in recovery, you’ll know what a scary and confusing time it can be. You’re likely to have a lot of questions going through your mind. Like, how long will it take to recover? Will I actually recover? What things should I avoid in case I make matters worse?
Intro 20:10
Doctors will explain things that obviously, you’ve never had a stroke before, you probably don’t know what questions to ask. If this is you, you may be missing out on doing things that could help speed up your recovery. If you’re finding yourself in that situation, stop worrying, and head to recoveryafterstroke.com, where you can download a guide that will help you.
Intro 20:33
It’s called the seven questions to ask your doctor about your stroke. These seven questions are the ones Bill wished he’d asked when he was recovering from a stroke will not only help you better understand your condition, they’ll help you take a more active role in your recovery, head to the website. Now, recoveryafterstroke.com and download the guide, it’s free.
Hilary 20:55
That’s kind of what the temporal lobe does. It’s really interesting.
Bill 20:59
So as a PT, or a therapist, you guys don’t really get involved. If you were to go down that path, you don’t really get involved with supporting memory and that type of thing. That’d be a different person wouldn’t it?
Hilary 21:13
Yeah. So your PT is really just going to get you walking again, get you moving your arms again, get you, you know, they’re going to be focusing on your body movement, your occupational therapist, maybe that individual that focuses more on, you know, getting some memory stuff back getting like that, you know, that organization back, like giving you tools to get through your day, as the new individual that you are, you know, and that’s really important.
Hilary 21:45
So like PT, and OT, occupational therapy, and then speech therapy. And those three individuals working together in like a Recovery Team for a stroke survivor is really important, especially if that individual has lost some, some speech due to, so that speech is also in the frontal lobe.
Hilary 22:10
So if the individual had a stroke in the frontal lobe, and it affected their speech, then a speech therapist would be really, really helpful to be able to get that back. So and that the good thing is that is that you know, it can come back, that’s, that’s something that’s really, really important to remember is that you can recover after a stroke, it’s, it’s different for everyone.
Hilary 22:31
Like we’ve said, 50 times, but, and the duration may be different somebodies recovery may be faster than another person’s, but that’s definitely not anything to read into, or to compare or whatever, that’s just the fact of the matter.
Hilary 22:46
But, working with those three individuals, your physical therapist, your occupational therapist, and your speech therapist, you know, if needed, that’s going to be able to really help, what’s going to be the most helpful, you know, and then whomever you kind of feel, I feel like, the bigger your recovery team is, the better, you know.
Bill 23:04
Yeah, it’s true. Sometimes though, it does get overwhelming when you have a lot of appointments, I remember having three or four appointments in a week, and then just domains that you can’t do anything else, you can’t get back to work.
Hilary 23:16
I’ll be pretty tuckered out after that.
Bill 23:17
Yeah, and if you’ve got to get to an appointment, my outpatient appointments were maybe, you know, a 15 minute drive from home, but getting ready to get to that appointment, because I wasn’t driving at the beginning, meant that I had to travel for an hour.
Bill 23:37
And then be there for an hour and then travel home for an hour. So you lose three hours. And that was a long, a long, whole three days a week, four days a week, out of your day. It’s really tough.
Bill 23:49
So I think I would have benefited from having them alternate. So one week, I would have had say PT and then the following week might have been better to have OT and instead of having three or four appointments a week, I only have one or two appointments a week that would have made a huge difference. But I know that the medical professionals what they like to do is make the most of that early recovery phase, and then cram in as much as they can there.
Hilary 24:20
That’s that’s really important, that sort of rash of like, let’s keep as much as we can. We’re gonna bombard you. And I do wonder, you know, I’m not versed in the current research, but I do wonder if we will maybe later on, you know, dive more into the research and figure out if that heavy of an intervention is as helpful as we as we believe it is because it is it’s very energy demanding on a an injured brain.
Hilary 24:50
You know, the brain requires so so so much energy, excuse me, and when it’s injured, it’s just It’s like expecting your arm, your broken arm to lift a milk carton, right? Like, that’s a lot it’s hard, you know.
Hilary 25:08
So if you think about it with your brain, like, you know, you’re bombarding it with all of this, these activities and these drills and all of this stuff from your, into your PT, you know, to your st. You know, when you haven’t done that before, and you’re injured, you know, it’s, it’s hard, but there’s definitely a reason for it. Right? Like, I’m not getting that, but it is hard.
Bill 25:27
Yeah, I think the reason is legitimate at the same time, I think it’s well worth re looking at that. Because when, when often they bombard you with that amount of therapy, and then pull the pin on it, and then it stops. Because they feel like okay, well we’ve done the three months worth of therapy in that window is when you’ll see all the recovery.
Bill 25:52
And then after that, we don’t expect to see too much more recovery. I think that’s very limiting. And slow and steady wins the race type of recovery, I think is the best one. And you can’t recover from stroke in the first three months, you just can’t it’s not possible, you can achieve a lot.
Bill 26:11
But I think that achievement of those things happens. Kind of regardless of how much effort you put in it, because it’s it’s kind of the window that it’s like the golden window of opportunity to get a lot back. And I think it just happens anyway. It’s really what I find stroke survivors struggling with is, you know, being 12 months and 18 months down the track when they are left alone.
Bill 26:37
And they want to recover, they use the fine motor movement of one of their arms or their leg or whatever, that’s when there’s no support. And I think that’s when it’s needed the most, because now those people are back in life most days in every day. And if they can’t get that back, they can’t experience the fullest version of themselves.
Bill 26:58
So I feel like, it’s great that recovery is bombarded at the beginning. But it starts and stops too abruptly, in my opinion needs to just smoothly and effortlessly kind of roll on. And if that means that the hours that you’re getting saved, in the first few months, you’re getting four or five hours a week, if those hours dropped to one or two hours a week, and then they were able to extend further along down the path.
Bill 27:30
That’s better, because in my opinion, like the brain still needs regular feedback of what to do to get better down the track that’s kind of my opinion. So I think it’s you know, it’s too abrupt, it’s too much. And then it’s too little. And that’s where the gap is. That’s what stroke survivors talk about often when I talk about there’s a lot of gaps when you leave hospital or therapy. So that’s interesting.
Hilary 28:00
It’s like left hanging, just like wondering what to do next afterwards.
Bill 28:04
Yeah, and there’s not a lot of information, there’s no information at all. That’s what I was struggling with, I was struggling with getting information, I was struggling to understand what part of my brain was impacted, because nobody told me what it was and what it did and what it meant.
Bill 28:21
And I didn’t think about looking it up, to be honest. But I’ve got curious about that later on. But, that’s the thing, they’re the gaps that I’m trying to fill with these interviews and the podcasts so that somewhere, somebody might get lucky and find that and find an episode that’s useful to them at the time, right? So you never know, things change.
The Brain Is Changing – Hilary Helt
Hilary 28:48
Yeah, definitely. I mean, and you’re 100% right about that it doesn’t happen in recovery doesn’t happen in just three months. It’s not, it’s not like when you stop, you know, PT or OT, that you’re done that you’re just like, okay, cool, like that, my brain is 100% back to normal, or my brain is just going to be whatever it is for that day, your brain is healing.
Hilary 29:09
I mean, I haven’t had a stroke, but my brain is changing every single day like that is how our brains are your neurons are either rebuilding or they’re breaking down, or your brain is changing every day.
Hilary 29:19
And it doesn’t matter if you’re in you know, therapy or not. And especially after a stroke when your brain is rebuilding and is, you know, figuring out how to make those neural connections again, to get basic body function back. You know, it doesn’t stop at that three month mark.
Hilary 29:37
So I think you nailed it on the head there. You know, it needs to be longer than three months. So we’re in different countries. I’m in the United States and you’re in Australia and our healthcare systems are a little bit different.
Hilary 29:51
But I know that in the United States, you know, they’re just gonna want money but also Insurance companies will only pay for some much. And so that’s kind of I think, where you’re really going to bump into the troubles of getting that. More therapy that’s definitely needed to move forward. You know?
Bill 30:15
I think it’s a conversation about you can still do therapy without paying for it, you know, if you just watch YouTube videos about therapy, exercises, all that kind of stuff you could still do, and that’s the thing, right? If you’re motivated enough, and funds are an issue?
Bill 30:34
Basically, my message is recovery doesn’t stop when they say it stopped, or when they say it’s done, when they say it’s over. It continues, It’s ongoing. And emotional recovery is also important. And so is physical recovery. And so is the mental recovery. Right? So there’s three pronged approach and perhaps more, but if you’ve left therapy, and all they focused on was getting you walking, and moving, and that type of thing, and they didn’t deal with the emotional impact than that, and that’s a problem for you.
Bill 31:07
Well, then that’s something that you need to also take care of. And so is the mental recovery, you know, counseling, all that type of stuff. And I understand that counseling might be a bit harder to obtain, because there’s a cost associated with that. But nonetheless, all these things need to be continuously sought after. And perhaps you need to get curious about what’s available for free, online, if for free is your thing.
Hilary 31:30
There’s alot available for free online, too. And, I mean, and I echo that 100%, I mean, you do need to have that little bit of a, you know, a starter in yourself to that motivation to get that information in that. Go in yourself. But there is so much information out there, a lot of it is really, really helpful, you know, stick to reliable sources, but you know, it’s all out there and a lot of it is free.
Hilary 31:33
And in each prong, too, right? So not just the, the mental but the physical, like different activities you can do to move on. So say you’ve, you’ve gained some mobility back and you’re ready for the next step. Well, that information is out there, you know, and then say you’re really struggling emotionally in recovery.
Hilary 32:16
There is a lot of resources out there too, that are free, or, you know, some reasonable cost, you know, it costs nothing to journal. Yeah, it’s nothing to you know, reflect go down, go down to the river or the lake or, or the, the woods or whatever, and just sit and just god man, why do I feel this way?
Hilary 32:35
And just kind of turn in, you know, that doesn’t cost anything. But, you know, it is tough, like, that’s easier said than done. And I do not mean to minimize that. But yeah, I just want to echo, you know, what you’re saying that, you know, all of that stuff is really important, and that it’s really, really available. If you need it, you know, it’s there.
Bill 32:54
Yeah, I think so. What does the parietal lobe do?
The Parietal Lobe
Hilary 32:59
So the Prado lobe is really interesting. I like the parietal lobe, because it has to do with touch, and the inch, so that we have these different neurons that like the very tips of our skin, that senses touch, and there, they just have like, these really crazy names. And like, there’s all these weird shapes, like one is kind of like a funny little oval, and it just, like gets smaller and smaller and smaller.
Hilary 33:22
Like there’s different neurons that like sense, pressure, and there’s different neurons that sense pain. And that all goes to your parietal lobe when you’re sensing all of that, and then there’s others that sense temperature. So like, if you’re going to, you know, touch that hot stove, right? That’s always the example why does everyone always use that example?
Bill 33:42
Because it’s so true, because it has that issue.
Hilary 33:46
Yeah. And then your neurons are gone to that parietal lobe, don’t touch that, that’s hot. And then so your prior to lobe is also going to interpret language and words, you know, so the parietal lobe and the temporal lobe kind of work together, you know, language wise.
Hilary 34:02
And then your product lobe has to do with your, your vision as well. So like, you know, if you have an A stroke in your product lobe, your vision may be affected, which is really kind of strange. That’s, that’s a hard one.
Hilary 34:16
I didn’t see any patients in my clinic with any vision problems after a stroke. But I would be interested to kind of, you know, hear how a stroke has affected somebody, his vision would be, I mean, that’s gonna be a hard one, right?
Bill 34:30
Yeah, I interviewed on the podcast, I interviewed a stroke survivor who had some serious vision issues. One of them was Maggie Whittum, and it was Episode 47. And the episode is called The Great Now What?
Bill 34:45
And Maggie’s vision is she has what how do I describe it like vibrating eyes?
Hilary 34:55
Like rapid eye movement?
Bill 34:58
Yeah, they just move up and down. All the time, and it creates blurry vision, it creates double vision. And then she sees, two of everything but very close together. So it’s kind of like a blurry version.
Bill 35:11
So that’s Maggie, Maggie is amazing. She’s in the process of writing and putting together a documentary about her experience. So that’s going to be a really cool documentary when it’s ready. So that’s Episode 47. The Great Now What with Maggie Whittum.
Bill 35:28
And so that was quite a while ago, still very relevant, obviously. But then most recently, there was an episode with Gloria Morgan, who had a brainstem pons stroke, Episode 117. And Gloria has some vision issues as well. So that’s an interesting episode to listen to, as well.
Bill 35:54
And she has also experienced tinnitus, which is an issue with the ear or the ringing in the ear. And some people will can actually make it a little better, I think, with some people with without drinking caffeine, so decreasing the amount of caffeine decreases the impact of tinnitus, and also there are hearing aids that can get rid of the tinnitus.
Bill 36:22
So I have a client. I have a coaching client who has tinnitus, and recently discovered that there was a hearing aid that he could put in his ear and it puts off a frequency that basically makes it go away, helps the hearing and also.
Hilary 36:39
So it kind of cancels it out?
Bill 36:40
Cancels it out, and then it’s gone completely. So there’s a couple of ways to help sort that out and help overcome it and get curious about that. If you’re somebody who’s experiencing that right now, I couldn’t recommend that enough, it was really cool to hear that he found a solution for that because it was really bothering him.
Bill 37:03
So the the parietal lobe is, sounds like a part of my parietal lobe was impacted, because I have those sensory neuron issues. So hot on the left side is a bit harder to register. And then sensation on my skin is a little bit of an issue. I feel a burning sensation and tingling all the time.
Hilary 37:27
Yeah, that sense of touch that got a little wonky, you know those neural pathways got affected in your parietal lobe.
Bill 37:34
Yeah, sounds like they got mixed up or wired differently or interfered with or something like that. So that’s like that, and also my left side is colder than my right side all the time.
Hilary 37:48
Oh, my gosh, how strange. How do you deal with that?
Bill 37:51
Yeah, well, you put your jumper on and you take it off every three minutes.
Hilary 37:56
On and off, on and off.
Bill 37:57
That’s what it is. And the left side gets really cold and sometimes hard to warm up. While the right side si doing quite well. And I’ve previously perspired on half of my body and not the other half.
Bill 38:14
So perspiration on my right side, but not on my left side.
Hilary 38:19
Wow, that’s wild. I haven’t heard of that one.
Bill 38:23
Yeah, that’s pretty wild. So when that happened, there was a bit of a shock. And I kind of realized I was perspiring, but didn’t know exactly that it wasn’t happening on my left side, until I went to wipe my forehead and it felt quite dry on one side. And then on the other side.
Hilary 38:42
Wild. Oh, my goodness. That is so strange.
Bill 38:47
That is really bizarre.
Hilary 38:48
Probably was, you know, the most fun thing to realize, right?
Bill 38:54
Kind of gets a bit fun at some point. Like at some point there’s so much.
Hilary 38:59
You have a good sense of humor about things.
Bill 39:01
You have to because there’s so much that you’re dealing with. And then when that happens, like, Man, that is nuts. That is crazy, because you’ve never experienced that before.
Bill 39:10
And no one knows what the body’s capable of doing. So it is regulating temperature differently at the same time on both sides of my body. And I don’t know why not. I can’t describe it.
Bill 39:23
But it’s cooling part of my body down while the other part is cool enough. I mean, that’s pretty intelligent. Even though it’s messed up, it’s intelligent, right? It’s still doing an amazing job of keeping me alive and and running all the regular functions. It just does it in a different way.
Bill 39:42
And if both sides of my body felt like my left side, then it would be normal. I wouldn’t notice the difference. But they’re difference so the right side is quite normal as it’s always been. Yeah, and the left side is different. So one of them is not worse than the other, it’s just that they’re different. And that therefore they get really, really noticed.
Bill 40:06
And I’m comparing, I’m always comparing, and I can’t avoid comparing, because it’s that part of, Okay, I’m feeling cold on one side, I need to warm that side up. But I can’t warm it up on its own, I’m going out, over, over warm up the other side. And it’s just this constant communication and Battle of balancing it and managing it. So you can wrap your head around it. And if you let it get to you it can be annoying.
Hilary 40:33
Yeah, you can’t let it get to you. But it’s, I can say that it’s that would be hard. But I do love that you brought that up books. That’s a really, really great example that just kind of talk about like, how just absolutely fascinating how just deeply integrated nervous system is.
Hilary 40:50
So there are so many neural pathways doing so many different things that, you know, you’re you’re feeling different temperatures on each side of your body. So it’s not like there’s one neuron one neural pathway that’s doing like that one thing that’s like, Okay, keep it cool, but you know, it’s not, it’s not one, it’s, there’s billions of neural pathways in our body.
Hilary 41:09
And you know, if just a few are a little wonky or messed up because of, you know, your stroke, then it’s going to have, an effect of, you know, one side of your body being one temperature on the other side of your body being another temperature because that one neuropathways, healthy and fine and was not affected, and the other is injured.
Hilary 41:29
So I think that that’s a really great example, to explain just how absolutely integrated our neural pathways are, how integrated our nervous system is into our body. It’s, it’s in every micro scopic, tiny speck of our bodies, it’s everywhere, you know, it’s controlling everything.
Bill 41:49
Yeah, and I imagine that the parietal lobe, my parietal lobe, therefore, in that area, it’s probably closer to the cerebellum, where it’s impacted. Because my, my bleed was near the cerebellum. So I imagined that and it was four centimeters in from my right ear, that the bleed happened, which is about two inches, I imagined something like that.
Bill 42:12
So the other side of the parietal lobe hasn’t been affected. So perhaps the fact that it’s on my left side of my head, the unaffected part of my head, therefore, it’s just running its regular neural pathways for the right side of my body.
The Occipital Lobe
Bill 42:28
So the left side of my head is not affected, the right side of my body is not affected. And it’s just, you gotta remember that switch. The regular routine, right? So anyway, that’s interesting. Yeah, so what does the occipital lobe do?
Hilary 42:46
So the occipital lobe is straight up, just vision. That’s what it takes care of, you know, just seeing color and light, and, you know, understanding movement and all that stuff. So that is vision, very simple for easy. The occipital lobe has the easy job. I mean, that’s saying that with a lot of just but yeah.
Bill 43:06
Yeah. So, if the stroke has impacted vision, and that’s happened elsewhere? I imagine there are more parts of the brain that are supportive or running, you know, pathways towards vision or something like that, if it’s not all just sort of happening there, because the occipital lobes in the back of the head and how does it like, go through all the parts as well?
Hilary 43:38
It’s kind of funny, right? It’s a strange way to think about it. So like, if you were to look like if you were to pull up an image of the brain and like look at like the, the nerves that go to your eyes, they’re kind of located a little bit farther back, they’re not like right here at the front of the brain that go like right to the eyes, they’re located kind of further back into the brain.
Hilary 44:01
So it’s not as much of a way as to travel if you think about it that way, because the very, they’re like in the far back and so like, they go straight into your eyes to say, anyway, I’m not very good at explaining that without like, giving like a picture.
Hilary 44:16
But pictures are very, very telling if you were to just Google like you know your nerves, nerves of the brain or nerves of the eyes, you would find it very easily and you would see what I’m talking about. It’s the occipital nerve. And it’s located a little bit further back in your brain.
Hilary 44:32
And if you look at the brain kind of as if you were to take it straight out of your head like this, and then look at it like that kind of like turn it down and look at it like that. You’d see the optic nerves right there a little bit further in the back of the brain and they and then they got their travel fourth into your eyes. Okay, you’re staying there long. They’re like a kind of like the longer too long pathways to the eyes.
Bill 44:56
So they can be there for impacted by him. Reach in a different part of the brain, or a blood loss supply in a different part of the brain could be peripheral damage of a different part of the brain, right?
Hilary 45:12
Yeah, so like, that’s what’s kind of tough about strokes, right is like say, like you have, you know, a blood vessel in the brain, you know, like in your parietal lobe that burst, but then the blood that that is like, you know, in your brain, and is kind of like just kind of trying to go, it has to go somewhere, right?
Hilary 45:29
So it could, you know, be pressing on to the other parts of the brain, and then affect those parts of the brain, even though, you know, they’re, they’re still getting blood supply from a different artery in your brain. But it’s affected because, you know, they’re getting that pressure from that, that blood pressing in, right.
Hilary 45:49
So strokes are just complicated in that way, right? Like, maybe you didn’t have your stroke there, but the blood traveled there and affected it in that way. So it’s hard strokes are hard, they’re, they’re tough, you know, and how you heal because that is a different injury.
Hilary 46:07
Because that part of the brain actually did continue to get blood supply, but it was just kind of squished, and it may heal better, or it may heal differently, because it actually still got that that oxygen from the blood supply so it’s tricky.
Bill 46:22
So that could be possibilities of peripheral damage, even though the occipital lobe is quite healthy and doing well. It’s just the other part of the brain that’s impacted. Therefore, that nerve coming from that occipital lobe to the eyes, is what’s impacted but down the road, it’s not impacted at the source.
The Cerebellum
Bill 46:44
Cool. All right, we are learning a lot. And this is probably one of those episodes that we’re going to need to listen back to a couple of times, I would say, what does the cerebellum do? And what’s its role?
Hilary 46:59
So the cerebellum is kind of like your, your baby brain, right? And, and it has to do with a lot really, the cerebellum is responsible for the maintenance of posture and balance. And then the coordination of voluntary movements, motor learning and cognitive functions.
Hilary 47:20
And we’re talking about things like like language again, right? Like you would think that like things are just kind of covered in the other parts of the brain. But the cerebellum has a part of language as well. So the cerebellum is kind of considered the part of the brain that like, Is Your Life source, right? But just because it is. It’s doing so much sound and I kind of leave it light like that.
Bill 47:47
Yeah. Okay. So the stroke, the bleed that I experienced, was near the cerebellum, I’m not sure which lobe it was near. So I’d say it was probably near the temporal lobe as well. Kind of makes sense. When I look at the brain 4cm in from the year.
Hilary 48:05
It’s like right they’re next to each other?
Bill 48:06
Yeah. Somewhere there. So definitely fine motor movement was an issue for me, I had to learn how to use my arm again and get it to come to my mouth so that I could put food in my mouth. Posture was a bit of an issue because I had to learn how to use to how to walk again and use my left leg again, and how to stand correctly how to run.
Bill 48:30
Not that I run marathons, I just run, for example, to get across the road if I need to that type of running. And you mentioned cognitive functions, I was really cognitively affected. Especially after the second bleed, I didn’t know who I didn’t know my name at one point and who my wife was.
Bill 48:52
I was unable to type an email would sit down and think that I’m typing an email. And it might have taken me a whole day to write three or four lines. And I wasn’t aware of the amount of time that I’d spent sitting there looking at the screen trying to put that email together.
Bill 49:11
I laugh now but it wasn’t funny at the time. You know, it was tough at the time.
Hilary 49:15
I’m sure, it must be so frustrating at the time.
Bill 49:17
Yeah, so it definitely makes the most sense. It was the one for me that was impacted the most. And yeah, cognitively I was, I’d start sentences and then not being able to finish them. And even today, sometimes I get stuck on certain words, like Where, where, where and where.
Bill 49:41
I don’t know which one goes where and when. So I know but I have to think about that I’m using the right one. And that wasn’t previously something that I did, I would quite easily find the correct way to use We are all, you know, where are you? Or where are you going? That type of thing.
Hilary 50:05
How was your balance afterwards. So the cerebellum is so you know, integral to balance, how is your balance?
Bill 50:11
Yeah balance is still a little bit off because of the sensation that I have on my left foot. And when I’m tired, so if I’m tired, I’ll find myself walking into doorways a little bit, you know, misjudging the distance between me and the doorframe.
Hilary 50:29
And that explains, you know, the knocking the glasses off of the table, too. That’s, you know, in your that’s controlled in your cerebellum as well. That’s all back there.
Bill 50:39
If I had bad run, I might knock over every second glass at the table. It’s not that bad. But it was at one point, we were going to lunch with some friends regularly at one point, and I was doing it almost every second time we were there.
Bill 50:55
And at some point, they just kind of got used to it. Oh Bill’s dropped something again.
Hilary 50:59
Like he’s made another mess. Okay, let’s just mop it up.
Bill 51:02
Pretty much, pretty much the fine motor movement again, you know, that makes sense. Because perhaps that I couldn’t grasp the glass correctly.
Hilary 51:14
Yeah. So that let’s differentiate the two, right. So for our listeners, unfamiliar with the difference between like your gross motor movements and your fine motor movements, your gross motor movements are just like moving a limb. And then your fine motor movements are like the very intricate movements that like your fingers.
Hilary 51:31
And your, you know, your feet to use to like, be able to grab that glass are able to just be able to pinch something between your two fingers, or just like move something with one fingers like that. Those are your fine motor movements.
Bill 51:44
So yeah, that’s the cerebellum. And then there’s the brainstem, right? So is the brainstem part of the brain or not?
Hilary 51:53
It’s part of the brain, but it’s like, it’s really kind of leading right into that spinal cord. So it’s just like the very tippy top of the spinal cord. But yeah, the brainstem is just kind of like that, you know, kind of, like I said, that, like, four way traffic stop, you know, it’s kind of like where it’s like really starting to direct that message.
Hilary 52:09
If it’s going to go to that, you know, first cervical nerve, or it’s going to go like thoracic mirror, you know, into like, telling your lungs to do something or, you know, going down to like your, you know, your abdominal nerves and stuff like that, you know, telling your guts to like, Hey, move that food down into the large intestine.
Hilary 52:28
So we can, you know, continue digesting or if it’s going to go down to a motor neuron and your leg cuz you need to walk forward, or what have you, you know, that’s kind of where that brainstem, the brainstem is at the start of it.
Bill 52:44
Okay, so it’s the brainstem is kind of the gateway, the bridge between the spinal cord and the brain. And it doesn’t have does it have any is it a blood flow thing? It’s a, what does it do? Does it have blood flow through a like a vein? Or is it just literally nerves? a pipe of nerves?
Hilary 53:08
You know, that I’m not super familiar with? I’m not sure. I know that every part of our body has, you know, blood supply. I am not sure about that exact answer.
Bill 53:23
Okay. That’s cool. So if I understand correctly, is the brain stem has also the pons and the medulla and a couple of other things. Are they part of the brain? Are they also part of the brainstem?
Hilary 53:40
There are the brainstem and there is the brainstem is kind of considered its own thing, really, but it is the beginning of the spinal cord.
Bill 53:48
Okay. Well, I think we’ve covered a lot. And I think this is a really full on and complex.
Hilary 53:55
Oh, and there’s so much you could have an entire podcast on the brain. The brain is exceptionally complex. And there’s a lot to it. It’s fascinating. It’s really great stuff. But yeah, we covered a lot.
Bill 54:07
Yeah. Fabulous. Thank you so much. I really appreciate it. So the anatomy nerd podcast is fairly new. Tell me a little bit about the type of people that you’ve interviewed so far. Yours truly.
Hilary 54:18
I know. You weren’t episode number five. Number four, number five. But yeah, it was really wonderful to have you on the podcast because, you know, the brain is part of our anatomy.
Hilary 54:30
And it’s interesting to cover the human body when it’s, you know, functioning well and then also when it’s not doing so great. So your episode was really wonderful. And also, you know, really helpful to just get stroke information out there.
Hilary 54:45
But then I’ve also interviewed some anatomy illustrators, that was a really, really fun episode. I’m just kind of talking to somebody who’s in the field about you know, when you look at these textbooks and websites and information, people pamphlets that your doctor has given you.
Hilary 55:01
All of those pictures, somebody drew them, somebody created them. So I interviewed a gal who is a medical Illustrator, she kind of, you know, described her path and her educational background and all that stuff, and what it all entailed to become a medical illustrator and that was really amazing.
Hilary 55:18
The episode that I had a lot of fun with was interviewing Frank Metter’s daughter. So for those of you who don’t know, Frank Metter was a surgeon and medical illustrator again, and he composed the anatomy Atlas, that pretty much the majority of medical students use to learn anatomy and physiology and all that stuff.
Hilary 55:44
I know, I used it to learn anatomy in college, and I had the pleasure of interviewing his daughter, and she wrote a book about Frank Metter, and told his story told about, you know, his, career at Cedars Sinai, and all of his medical illustrations and all of that, and that was really amazing. I really enjoyed my conversation with her.
Bill 56:10
And is his work still relevant? Was a really well done that it’s still current?
Hilary 56:16
Yes, yeah. 100%. Yeah, it’s still used today. Yeah, it’s pretty great. And they’re really beautiful images. I think that one of the things that I just loved about Frank Metter is that, you know, it’s accurate. It’s, and it’s still used today, because it you know, who is only only drawing these, illustrations, you know, maybe a couple of decades ago, not, it’s not like he was doing it, like, hundreds of years ago.
Hilary 56:44
And he didn’t know anything about the body, like, no, they’re definitely recent enough that they’re accurate. But he just had this really amazing way of putting, you know, that human emotion and that human personality that the human element into the illustrations, and it goes a long way.
Hilary 57:01
You know, it kind of teaches that student, it reminds them that, hey, you know, your patient, whatever that may be in whatever medical field, you’re working in, that you’re working with people, you know, not just a medical illness or what have whatever you’re dealing with.
Hilary 57:19
You’re dealing with a person and remember that and that, you know, everyone deserves respect and all of that. So he conveyed that in every single one of his illustrations. And it’s amazing that he was able to do that. It’s pretty cool.
Bill 57:32
Yeah, sounds interesting. So where can people find the podcast if they want to, to reach out and connect?
Hilary 57:39
On every podcast platform and app so you name it. It’s in Apple, it’s in Google. It’s on Spotify. It’s on Stitcher, it’s on all those things.
Bill 57:53
On the socials? Where will they find you on the social medias?
Hilary 57:57
I am on Instagram, mostly. I’m mostly active on Instagram.
Bill 58:00
Fabulous. Well, Hilary Helt thank you so much for being on the podcast and explaining to us a little bit about the brain are really appreciate it.
Hilary 58:10
Thank you so much for having me, Bill. It was really, really wonderful to get to talk to you and nerd out about the brain a little bit.
Bill 58:16
Thanks so much for joining me on today’s recovery after stroke podcast. I hope you enjoy the episode. Do you ever wish there was just one place to go for resources, advice and support in your stroke recovery?
Bill 58:28
Whether you’ve been navigating your journey for weeks, months or years, I know firsthand how difficult it can be to get the answers you need. This road is both physically and mentally challenging from reclaiming your independence to getting back to work to rebuilding your confidence, and more.
Bill 58:46
Your symptoms don’t follow a rulebook and as soon as you leave the hospital you no longer have the medical professionals on tap. I know for me, it felt as if I was teaching myself a new language from scratch with no native speaker in sight. If this sounds like you, I’m here to tell you that you’re not alone.
Bill 59:03
And there is a better way to navigate your recovery and build a fulfilling future life that you love. I’ve created an inclusive supportive and accessible membership called recovery after stroke. This is an all in one support and resource program and it is designed to help you take your health into your own hands.
Bill 59:25
This is your guidebook through every step in your journey from reducing fatigue, to strengthening your brain health to overcoming anxiety and more. To find out more and to join the community just head to recoveryafterstroke.com See you on the next episode.
Intro 59:45
Importantly, we present many podcasts designed to give you an insight and understanding into the experiences of other individuals opinions and treatment protocols discussed during any podcast or the individual’s own experience and we do not necessarily share the same opinion nor do we recommend any treatment protocol discussed.
Intro 1:00:02
All content on this website at any linked blog, podcast or video material controlled this website or content is created and produced for informational purposes only and is largely based on the personal experience of Bill Gasiamis. The content is intended to complement your medical treatment and support healing. It is not intended to be a substitute for professional medical advice and should not be relied on as health advice.
Intro 1:00:25
The information is general and may not be suitable for your personal injuries, circumstances or health objectives. Do not use our content as a standalone resource to diagnose treat, cure or prevent any disease for therapeutic purposes or as a substitute for the advice of a health professional.
Intro 1:00:40
Never delay seeking advice or disregard the advice of a medical professional your doctor or your rehabilitation program based on our content if you have any questions or concerns about your health or medical condition, please seek guidance from a doctor or other medical professional.
Intro 1:00:53
If you are experiencing a health emergency or things you might be call triple zero if in Australia or your local emergency number immediately for emergency assistance or go to the nearest hospital emergency department medical information changes constantly. While we aim to provide current quality information in our content. We do not provide any guarantees and assume no legal liability or responsibility for the accuracy, currency or completeness of the content.
Intro 1:01:17
If you choose to rely on any information within our content, you do so solely at your own risk. We are careful with links we provide. However third party links from our website are followed at your own risk and we are not responsible for any information you find there.